This is making me wonder about some other “alternative” remedies that have been dismissed by the US medical profession and mass media, sometimes with studies claiming to disprove hopeful early signs of effectiveness.
Megadose Vitamin C? Remember the controversy about Dr. Linus Pauling?
Laetrile (apricot pits) for cancer, popular in the 1960’s and 1970’s, now banned by the FDA?
Bleach?? Chlorine dioxide is chemically a member of the bleach family. It’s been marketed as a supplement known as “MMS” (Miracle Mineral Solution) and attacked by the FDA as hazardous and worthless.
But, here’s Andreas Kalcker claiming that a pilot study in Ecuador, claiming that 97% of >100 patients had remission of severe coronavirus symptoms within 4 days. This compares very favorably to Raoult’s claim of 91.7% positive clinical outcome and viral clearance within 10 days in his 1061 patients treated with HCQ+AZT.
Kalcker also talks about the very small doses of chlorine dioxide used in the study, compared to the LD50. In comparison to HCQ or even tylenol, the treatment seems to have a very safe therapeutic index ratio.
Could this possibly be true? Everyone mocked Trump about his “bleach” comments, so is he going to get the last laugh?? (Actually I think Trump was talking about lysol.)
https://lbry.tv/@Kalcker:7/100-Recovered-Aememi-1:7
Who are their backers? Or did they just decide to make some side money? Who paid for the study? Who benefits–besides Gilead? Why does it seem that old(er) people are getting the shaft? Or is that really the case or just another morsel of partial information we’ve been fed? This cast of players is beginning to resemble ‘War and Peace’; I need not only a list of those involved, but a character tree. I can’t believe this lot are cohesive–but who is playing whom in the mess? And how many who(s) and whom(s) are there? I keep thinking that we shouldn’t attribute to malevolence that which can be explained by greed and stupidity, but I don’t think that is always true.
Enquiring minds want to know… Maybe the enquiring minds need to become the inquiring minds?? But what authority can we trust to make the inquiry?
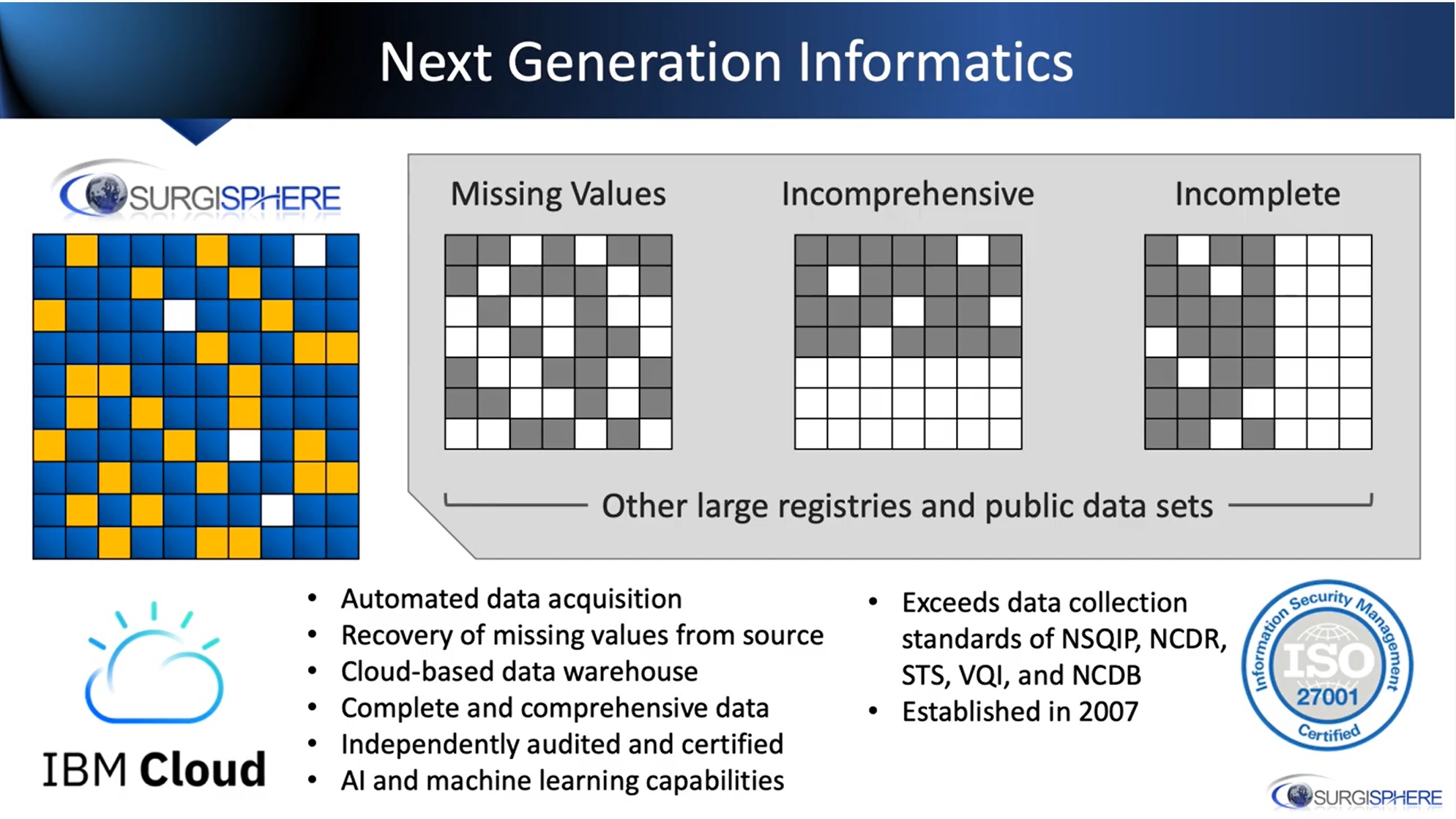
There are a few videos on Youtube from Surgisphere. One of them is Sapan Desai talking about his, “next generation informatics system”. Artificial intelligence (AI) and machine learning (ML) are indeed powerful tools that are at the forefront of computing… something I well understand from the semiconductor hardware side of the table… but I have to say my ears really perked up when I heard Desai say the portion of the sentence in bold below, which I transcribed from the linked video;
"We've created a next generation informatics system that uses a lot of automated data acquisition, we're able to recover missing values from the source, and using artificial intelligence, machine learning, and natural language processing, we've created what is today the worlds most complete, comprehensive, and accurate health care data set". source: https://www.youtube.com/watch?v=au73eCxtZp0The chart that was being shown during this statement is presented herein. This guy can really fling the buzz words around.. but based on all the breaking news around this company and the Lancet paper they were behind, you really have to question much of what is said in the transcribed statement, which BTW dates back to Mid-March. For instance, we have seen that there are many hurdles to getting data from hospitals.. pesky ethics boards and such.. hence the concept of, "automated data acquisition" hardly seems possible. It also sounds like they are basically letting the computer make up at least some of the data and hiding this behind lofty terms like AI and ML. I will be interested in Chris' take here...
no thanks, Jan. I don’t think A full-fledged eco-socialist Marxist revolution would bring anything but more death and misery. Hasn’t Marxism produced enough of that already?
Yet another life-saving protocol is being ignored & suppressed:
According to the article, efforts by Dr. Pierre Kory — medical director at the Trauma & Life Support Center and a faculty member in the Division of Allergy, Pulmonary and Critical Care Medicine in the Department of Medicine at the University of Wisconsin School of Medicine and Public Health — to share the Front Line COVID-19 Critical Care Working Group's4 (FLCCC) successes with other health care professionals have so far come to naught. Kory was one of five doctors participating in a May 6, 2020, roundtable discussion5 on COVID-19 with ranking senate committee member Gary Peters, D-Mich. In his testimony, Kory states, in part:6 "I want to start by saying that I am part of a group of physicians which include several of the most highly published and well-known critical care experts in the country and world (Drs. Paul Marik, Umberto Meduri, Joseph Varon and José Iglesias). In response to the COVID crisis we formed the Front-Line Critical Care Working group …
Members of our group have now treated in excess of 100 hospitalized patients with our treatment protocol. Nearly all survived. The two that died were in their 80s and had advanced chronic medical conditions.
None of the patients have had long stays on the ventilator nor become ventilator dependent. The patients generally have a short hospital stay and are discharged in good health …
Our protocol has been out over four weeks. It is not unique, in fact, we are not alone in what we propose or have been trying … In fact, we are seeing an increasing number of similar protocols with nearly identical therapeutics come out from various institutions and countries, including the Italian guidelines, Chinese guidelines, Yale protocol, Montefiore protocol and others.
We are doctors, trained to diagnose and treat illness, we are experts in our field with decades of experience and hundreds of publications … We have clearly devised an effective treatment for use, prior to the publication of randomized controlled trials.
Those trials are critical for sure, as they will help us further refine and/or perfect our treatment doses, durations, and indications, but waiting for the perfect is and will be the enemy of the good, which we are already achieving … We just want to save lives, and we know how to do it." The MATH+ protocol7 calls for the use of three medicines, all of which need to be started within six hours of hospital admission:https://articles.mercola.com/sites/articles/archive/2020/05/29/dr-paul-marik-critical-care.aspx?cid_source=dnl&cid_medium=email&cid_content=art1HL&cid=20200529Z1&et_cid=DM547465&et_rid=882299015Optional additions include thiamine, zinc and vitamin D. In addition to these medications, the protocol calls for high-flow nasal oxygen to avoid mechanical ventilation, "which itself damages the lungs and is associated with a mortality rate approaching nearly 90% in some centers," Kory notes.8 Together, this approach addresses the three core pathological processes seen in COVID-19, namely hyperinflammation, hypercoagulability of the blood, and hypoxia (shortness of breath due to low oxygenation).
- Intravenous methylprednisolone, to suppress the immune system and prevent organ damage from cytokine storms — For mild hypoxia, 40 milligrams (mg) daily until off oxygen; moderate to severe illness, 80 mg bolus followed by 20 mg per day for seven days. On Day 8, switch to oral prednisone and taper down over the next six days.
- Intravenous ascorbic acid (vitamin C), to control inflammation and prevent the development of leaky blood vessels in the lungs — 3 grams/100 ml every six hours for up to seven days.
- Subcutaneous heparin (enoxaparin), to thin the blood and prevent blood clots — For mild to moderate illness, 40 mg to 60 mg daily until discharged.
Dr. Martenson,
Have you seen this report?
https://www.santafe.edu/news-center/news/new-model-predicts-peaks-covid-19-pandemic
This might better explain the early numbers coming out of China than your earlier accusation of malicious manipulation of data. I suspect if China were still manipulating its numbers, we’d know that from reports of known people becoming infected, or of infections coming from China (as happened with Iran).
I’m sure their numbers are way lower than the real thing. Probably not so much so as Russia, and certainly not so much so as Brazil (where I am now, and where inadequate testing means a possible error of 7x(!) , and perhaps not even as much so as in the US today.
But this new mathematics may be a better explanation than the earlier speculations.
Seriously, you can’t make this up.
The WHO is now recommending for healthy people that they only wear a face mask when caring for known CV-19 patients. IMO, the WHO isn’t simply incompetent. The WHO is instead an extremely corrupt organization that elected to side with China, and it’s main purpose now is to be the primary propaganda mouthpiece for China. They are not just corrupt, but they are downright evil.
MSN article
It’s called dog shit.
MMR does not cause Autism!
and
The original MMR shot did not cause aseptic
meningitis! Oh wait…
https://pubmed.ncbi.nlm.nih.gov/10707922/
I know the vaccine debate is a hot button one, and I don’t care what you believe to be true. Just don’t tell me I’m a nut job for having serious concerns about the “safe and effective” meme. Especially when it involves 8 week olds.
Trust has gone, and, we’ll all pay the price…
In the UK it is utterly ridiculous. One way systems everywhere, Perspex everywhere and still, less than 1% wearing a mask.
https://www.medicineuncensored.com/a-study-out-of-thin-air
Read the rest at James' website.A Study Out of Thin Air
by James M Todaro, MD (Columbia MD, @JamesTodaroMD)
May 29, 2020
Misinformation is bad. Misinformation in medicine is worse. Misinformation from a prestigious medical journal is the worst. Herein is a detailed look at the controversial Lancet study that resulted in the World Health Organization ending worldwide clinical trials on hydroxychloroquine in order to focus on patented therapeutics....
Is another reason why I love Peak Prosperity. This is like watching an episode of “Lt. Joe Kenda, Homicide Hunter” unfold in real-time, as the collective brain trust eviscerates shoddy science. =)
Don’t agree on the assessments of accurate reporting. Do believe the good old Chinese zapped the numbers to begin with, but also know what efforts they’ve put in to stop the spread and help other countries. Do not put much credence in Russia fudging stats - that horse is old and worn out. Cheers.
What’s most disconcerting is who, like veritable dominoes, a number of governments and organisations reacted as if on cue. That’s just despicable.
My thought exactly. Its not that numbers were not so much in disagreement. In fact they were in too much agreement. The hospital count does not correspond with the possible hospitals for the counts in the system. The only way to get those counts is to use one fictitiously stolen from those figures. And I agree, there is a lag in the reporting in which they(authors) admit. But the numbers agree with disposition of completed case work by reporting attending MDs at the time of authoring… accounting for no lag in reporting time between case count… history, presentation, treatment, and resolution recording… especially considering each hospitalization is greater than 2.5 weeks on average. Opps… cant even fake the numbers correctly.
Surgi wrote a cryptic response.
https://surgisphere.com/2020/05/25/lancet-paper/
this has to be one of the most dismaying videos I have seen in the past 20 years. to think that somebody would work to publish a study with such flawed methods, and to have that result then quickly blasted all over the world media, with the attendant consequence, is just sad beyond belief.
thanks Chris (and thanks ‘akancide_is_real’ whoever you are) for shining a light on this
We are all familiar with Dr Raoult’s study. They easy trashed that as a garbage study… to discount that work - And with no real explanation of what was wrong with it// Except they “believe” that the inclusion criteria and triaging of patients in regards to ensure patient safety was inadequate/?? what that is subjective not objective. And I would like to know how many patients who received the drugs had adverse events/. its looks like they did much better than those who did not…// So when these organizations put their "sh^&^ on the line… and give no exacting answer… they are part of the conspiracy… I would love to interview these chumps as a journalist… I would eat them alive , I dont understand where real journalism exists today…
In a statement last week, the International Society of Antimicrobial Chemotherapy (ISAC) said the study in question did not meet its standard—but did not go into many details as to why.You know why they didn't go into detail.. Because its not about the study .., its about the politics..
In applications that involve forecasting the future (meteorology for instance), a separate machine learning model is sometimes to predict the missing values in the historical data set that contains all sorts of variables include the one we are trying to predict. The historical data set, now consisting of some real observations and some “simulated” observations (i.e. guesses) can now be used to train a model to predict the future values of variables we are trying to forecast. This forecast can be more accurate than one generated by simply throwing out data from times with missing observations. This can be true even if the attempts to fill in the missing data are not very accurate - as they usually are.
But to do this in a retrospective medical outcomes study where the most important outcome is death? And to base real-world decisions on the results? That sounds very risky to me - and wide open to manipulation.
QB-
The historical data set, now consisting of some real observations and some "simulated" observations (i.e. guesses) can now be used to train a model to predict the future values of variables we are trying to forecast.Oh I get it! Here's my guess as to how that works. Let's say you have a bunch of patient records that are missing whether the patient is a smoker or not. You have a bunch of patient records that do have this filled in, as well as a lot of "other information." You train up a model that can predict, from the "other information", whether or not the patient is a smoker. You test it against these complete record-patients to make sure this model (mostly) works. Then you execute the smoker/non-smoker model against the records with the missing "smoker/non-smoker" entries. You come up with your guesses, and fill in the blanks. Presto - you now have records with patient smoking status "correctly" filled in. And - mostly it will be right. More right than wrong anyway. Hopefully. Depending on how representative your training set is of the entire global patient population. [That last one: the critical assumption.] Rinse, repeat, for every missing column for every patient record. I do not think they are being clear with their customers (or us) as to what they are actually doing, however. They have patchy, incomplete data where they have "filled in the empty bits" using a collection of AI models they've trained up, which "hopefully" have been trained using representative global data. How many empty bits have been filled up by AI? How many are authentic records? What were the training sets? We don't know. And they aren't telling us. Here's how this goes wrong: Let's say you train up your "smoker/non-smoker" model on just US patient data, with complete records from a few select hospitals in the US. Then you attempt to "fill in the smoker/non-smoker blanks" for people in Africa/Europe/Asia - with different smoking prevalence, different diet, different climate, different average BMI, different local pollution, and who knows what other confounding factors - your model may well just spit out errors that you will never detect. That's because your model has been trained to detect "meaningful smoker indicators" in one population that simply do not generalize globally. The models will never tell you this. They will happily spit out wrong answers from now until the sun goes cold. Models are only as good as their training set. Do we get to see the training sets on which the models were trained? No. Do we even know how many data items were "filled in?" No. "It's proprietary."