For what it’s worth, a guy in the linked thread did a back of the envelope reworking of the stats in the Boulware et al HCQ post-exposure prophylaxis study. His reworking indicates that the study data did show a very large decrease in people who developed symptoms if they started HCQ within 1-2 days after exposure (the study reported the stats for people who started within 1-4 days after exposure altogether but broke it down further in table s6 in the Appendix). Unfortunately, the confidence intervals are large due to the small number of participants. If interested it’s toward the bottom of this thread under ‘Bob’s’ comments on 5 June https://blogs.sciencemag.org/pipeline/archives/2020/06/04/hydroxychloroquine-for-avoiding-infection.
Looking at table 1 in the Boulware article, I think the similarities between the contol and test group are suspiciously similar for a random study.
Hi Robie,
I planted Beauregard also…got mine from Tatorman. Been in 3 weeks…Have 3 varieties total. Also Vardamum (sp?) and one other… 500 plants total. Sweet potatoes and butternut squash are my storage crops.
Glad you are well!
TamHob-
For what it's worth, a guy in the linked thread did a back of the envelope reworking of the stats in the Boulware et al HCQ post-exposure prophylaxis study...Yeah I saw a similar comment on a twitter feed - did the math myself - 1-2 days: 9.6% infections (HCQ) vs 15.4% infections (placebo). I posted my detailed bits on Jim's HCQ thread. If they had more "day 1" participants I suspect they would have found it to be even more effective. I'm guessing, as with HIV PEP, "every hour counts."
Looking at table 1 in the Boulware article, I think the similarities between the contol and test group are suspiciously similar for a random study.I pointed that out several times in reviewing their demographics data. But I didn't want to cast aspersions on a mere suspicion. However, given that this wasn't a propensity matched study - just random assignment - I don't believe their n was large enough to give us such eerily similar columns for HCQ and placebo. It just...feels too clean.
Dr. M, Where the study shows 13% developed COVID, but only 3% were confirmed by PCR, I take that to mean 3% of total study. Thus, 3%/ 13% = 23% of (reported) infections were confirmed by PCR. I find that % change in a value that is a percentage is often confusing, and authors are rarely clear. In this case, if only 3% of infections were confirmed by PCR, that might really call into question the validity of the study. So, if my hypothesis is right, it doesn't materially change the punchline, but adds a tad bit of credibility to the testing. Thoughts?You make a good point, and here's how I was thinking about it. (1) We know that a very large proportion of people who are exposed to covid remain totally asymptomatic. Still they can be detected via PCR testing. With this in mind, the total proportion tested matters I think. Especially if it turned out to be the case that HCQ - or placebo - somehow had greater or fewer proportions of these exposed and infected but asymptomatic people. (2) Besides the 3% tested, the other 97% were evaluated on the basis of self-reported symptoms. It does help that of the people deemed to be probable/possible (P/P) Covid 23% were confirmed by PCR. What I couldn't find in the discussion, but I may have missed, is if it ever happened that someone was deemed possible/probable but then was excluded because their PCR came back negative. Did this happen? Were these study subjects then just chucked back into the negative pile? That would be good to know as it would allow us to very roughly gauge their false positive rate. That aside, they had a very low rate of (self-described) symptomatic people who were not classified as covid P/P.
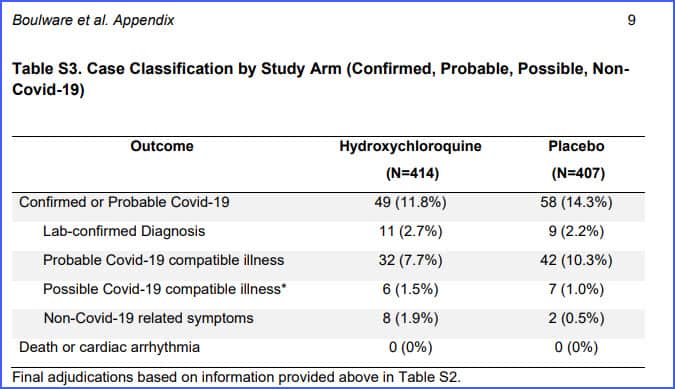 Just 1.2% (combined, weighted) or 10 people were deemed to have symptoms but not be covid P/P which seems odd to me. (By the way, it bothers my inner OCD that the Non-Covid related symptoms row is indented when it shouldn't be) out of 117 symptomatic people 107 were deemed Covid-19 and just 10 were deemed not. Does this make sense? Would we expect just 10 people out of 821 to have some sort of symptoms during cold/flu season? I don't know...but my gut says that's low.
You know what would really help here? Testing!
Bottom line: I think it's highly relevant that just 3% of the total were tested.
The more I sit with this study, the less it tells me and the more questions I realize I still have.
Just 1.2% (combined, weighted) or 10 people were deemed to have symptoms but not be covid P/P which seems odd to me. (By the way, it bothers my inner OCD that the Non-Covid related symptoms row is indented when it shouldn't be) out of 117 symptomatic people 107 were deemed Covid-19 and just 10 were deemed not. Does this make sense? Would we expect just 10 people out of 821 to have some sort of symptoms during cold/flu season? I don't know...but my gut says that's low.
You know what would really help here? Testing!
Bottom line: I think it's highly relevant that just 3% of the total were tested.
The more I sit with this study, the less it tells me and the more questions I realize I still have.
Study published in Lancet has been retracted
James Todaro, MD, also provides worthwhile information on his Twitter-account regarding the coronavirus and hydroxychloroquine. What he says is in line with what Chris is saying. In my opinion, he’s worth checking out:
https://twitter.com/jamestodaromd
Regarding statistics and the coronavirus, the information in below might provide some very interesting insights:
Lies, Damned Lies and Coronavirus Statistics
“The numbers are in on the great Covid-19 pandemic . . . but unfortunately those numbers are unreliable. From mendacious models and puffed-up projections to dodgy death data and tainted tests, today on The Corbett Report James highlights what the accredited scientists and award-winning researchers are saying about the pandemic pandemonium of 2020.”
https://www.corbettreport.com/lies-damned-lies-and-coronavirus-statistics/
One possible explanation for the similarities in the two groups is the internet recruitment. I suspect what happened was that the link to sign up for the study was circulated among friends, very possibly within closed facebook groups or other similar groups on other platforms. The link may even have been shared via email.
I can even imagine a scenario such as “hey, friend- I know you’ve been exposed to COVID and want HCQ but you can’t get it, here’s a study where you might be able to get it- sign up with this link”.
That HCQ study based off of self-reported data bothers me. First of all, the % of participants with comorbities is much less than the general population such as those with hypertension. Both arms of the study were way too healthy. That raises two questions in my mind. First, how accurate was the information on comorbities in the first place? This makes me inherently question all of the self-reported data. Second, it is already known CV-19 greatly spares those without chronic illnesses. Ideally, treatment research should be focused on those who are more affected by CV-19. Doing a study in healthy 25 year olds is not going to be very beneficial, but doing it on 50 year olds with comorbities would be very beneficial. This study was slanted towards a group of relatively healthy individuals for some reason. The meat of this study was based of off very subjective symptomatology from self-reporting. From my experience in caring for patients for close to 20 years patients oftentimes have difficulty answering seemingly simple yes/no questions when I’m taking their history. Many times it goes something like this… “Were you short of breath?”…”Hmmm, I’m not sure. I could have been. I think I might have had a little heaviness in my chest, but I’m not sure if I was having difficulty breathing. I really don’t know.” Our minds can easily play tricks on us. Whatever you do don’t think about your face itching. Sure enough, many peoples faces will itch all day long if they keep thinking that thought. As Chris has mentioned there was a gross lack of testing, and consequently a gross lack of objective data in this study. When there’s potential error multiplied by potential error multiplied by potential error, etc. then any potential conclusions can get pretty wonky fairly quickly. I don’t feel there is any meaningful conclusions that can be drawn from this study. It’s just another piece of non-information.
dryam-
The PEP study participants were recruited (I believe) on social media, so I’m guessing the audience there would skew younger. I saw Boulware reference a facebook ad he placed, for instance. And he posted tweets every day or so recruiting people there too.
His twitter feed:
https://twitter.com/boulware_dr
I got the sense he had to scrounge around for funding, since NIH was unwilling to come up with a penny. [That, from his twitter feed also]
Anyone else experiencing it? And I don’t me information overload. I am talking about at first yeah, masks, preps, distancing - we can do this. Now, even though you know it still needs to be done, you start to say, this is taking a lot of extra effort to do things that should come easy… It becomes exhausting, maybe its just me because i am disabled.?
when you dont actually test the majority of people and only go by (subjective) clinical presentation, the study becomes pretty much useless.
A Twitter thread about the failure of science, wrt HCQ.
The Recovery trial has a home page, which has a link to the statement about HCQ. But it looks like only hospitalized cases were enrolled, so fairly useless as an anti-viral and hardly surprising that no effect was seen. No mention of zinc, no use of azithromycin in combination with HCQ (az was a separate treatment). The bad science continues.
This is from Andy Borowitz in the New Yorker.
https://www.newyorker.com/humor/borowitz-report/trump-optimistic-about-winning-nobel-prize-in-medicine?utm_source=facebook&utm_medium=social&utm_campaign=onsite-share&utm_brand=the-new-yorker&utm_social-type=earned&fbclid=IwAR3dBcfcJDMzi9V55S8h3-2QW-Yq_THXHmODdpa1JT1zQqrGniMi84fp8aI
I’ve been thinking about adding sweet potatoes to my garden, OliveOilGuy, and your post tipped me over; I just place my first order! Here in the mountain spine of central Vermont, it’s just now planting time for main season field crops, so the timing’s good, too.
About the Lancet study:
“A data analytics firm behind an influential - and now retracted Lancet study which concluded that Hydroxychloroquine is dangerous, has one employee and is headquartered in a residential house just west of Chicago. Yet its bogus data prompted the World Health Organization, the UK and France to halt clinical trial programs involving the controversial drug used to treat COVID-19.”
https://www.zerohedge.com/health/dodgy-data-firm-behind-retracted-hydroxychloroquine-study-raises-questions-over-haphazard
I would like to know what the current thinking on this site in terms of what protocols people are currently using for making things safe that come into the house. For example, how long do you wait to:
-open your mail after you get it out of your mailbox?
-open a package from Amazon?
-handle non-perishable food items from the store?
In our house, the answer to all of the above is 9 days, unless something absolutely is needed before then, in which case it is properly cleaned (for example, all veggies get soaked in a light bleach solution for at least 20 min before being dried and put in the fridge).
And yet, when I speak with my friends and family, who don’t follow this site, they think I’m nuts. Even though the longest the virus is known to survive on a surface is 9 days and I’m following the precautionary principle, which is to take the precautions until it’s proved that they are not needed. Is there now enough evidence now to prove we don’t have to wait 9 days- for things like mail and groceries?
Early podcasts and videos from CM indicated to treat everything like it was covered toxic waste. Then this study came out on April 16th from NEJM saying that Covid-19 can only survive on plastic up to 72 hours, stainless steel up to 48 hours and cardboard up to 24 hours. Yet discussions on this site were still indicating people were waiting 9 days, at least for rotating masks. It was not clear to me if people adjusted the time frames for other things like mail (1 day?), packages (3 days?) or non-perishable groceries (3 days?)
Then, May 29th, this article came out indicating that the CDC is now saying that it’s not nearly as likely that it’s transmitted by surface contact as we originally thought. Is this more BS from the CDC? Or can we relax our protocols? Is there enough evidence now to prove it’s ok to wait less than 9 days? I would greatly appreciate input from Chris, Adam or others on this site if you have adjusted your thinking about surface contagion at all, especially in the last month or so. Is there any other evidence that has come out recently about this topic that I am missing?
I believe that the “9 days” principle was because of prior research into how long other coronaviruses remained viable on different surfaces, with 9 days being the longest. However, I seem to recall that more recent work with SARS-Cov-2 suggests that 3 days is the longest it survives, though I don’t recall the material concerned.