Zelenko: HCQ deniers are guilty of mass murder
https://www.youtube.com/watch?v=U4Qubuhs_Pc
Interview with Dr. Zelenko.
Also, is it known if immunity is protective against new mutations of the virus, or only for the original strain?
Well right after posting my question I watched Chris’s new video. Voila he goes into it in great detail.
Answer not much and not too long apparently.
Interesting tool explained on the new Medcram video.
https://profile.covid-age.com/calculator
https://www.henryford.com/news/2020/07/hydro-treatment-study
Full text of publication
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
I agree that if all other things remain equal, lock downs do not change the area under the curve (the integral of cases over time, i.e. total infections) but lower the peak numbers per day and spread out the total cases over a longer period. This is mathematically correct. However, if quarantine reduces transmission, does R actual remain the same? Could not quarantining sick people deprive the virus of new hosts?
I am curious about the assumptions regarding building herd immunity. I wonder if there might be something different about SARS Cov-2. I too have seen data suggesting some people have limited T cell mediated immunity based on previous exposures to other coronaviruses. However, I have also seen reports of people getting COVID a second time, just as badly as before. Is this because the antibody response is weak? Or, could this be because we have a new mutant D614G circulating now? If the latter, vaccines are going to be hit-or-miss just like the flu shots.
I’m curious, I read about asymptomatic spreaders. Forgive my ignorance, but if people are asymptomatic, how do we actually conclude they are responsible for spreading the disease? I read a paper about this that estimated asymptomatic spread and it seem to be based on an algorithm (So depends whether assumptions were valid).
Perhaps we have a chance to change the course of things now that one of the Henry Ford Hospital studies is out.
I hope they manage to complete their prophylaxis study on nurses, apparently the hospital admisssions have dropped ( agood thing) But fewer care providers to enroll as a consequence…they may have convince hospitals outside their system to join the investigation.
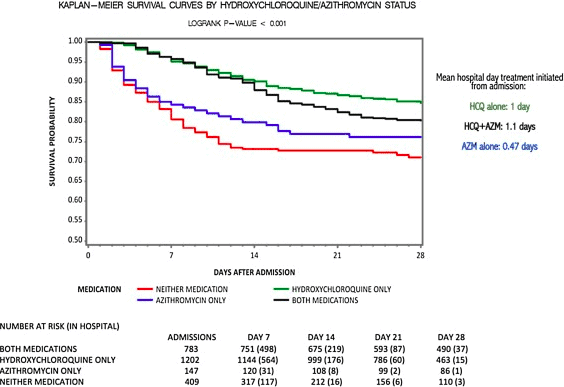
Henry Ford Hospital System HCQ and Azithromycin Study of Mortality (in patients)
Conclusion
Hydroxychloroquine provided a 66% hazard ratio reduction in in-hospital mortality, and hydroxychloroquine + azithromycin 71% reduction when compared to neither treatment (p < 0.001)
So this is a very strong positive study for HCQ.
Methods
Consecutive patients admitted with COVID over an 8 week period, age > 18, did not die within 48 hours, retrospective, unblinded, comparative-cohort study driven by protocol that included both steroids and tocilizumab. If baseline EKG was > 500 ms, patient was judged to be high cardiac risk, then HCQ and Azith were not given. HCQ was reserved for only the most severe COVID cases and for those without elevated cardiac risk. ---Outcome
In hospital mortality---- Crude Results
-
Total Mortality: 18%
-
HCQ + Azith: 20% <-- higher crude mortality as most severe cases were given HCQ.
-
HCQ alone: 13%
-
Azith alone: 22%
-
Torsade de point arrhythmias: none
- Respiratory failure: 88%
- age>65 years HR:2.6
- white race HR:1.7
- CKD HR:1.7
- reduced O2 saturation level on admission HR:1.5
- ventilator use during admission HR: 2.2
-
The combination of hydroxychloroquine + azithromycin was reserved for selected patients with severe COVID-19 and with minimal cardiac risk factors.
-
A hydroxychloroquine was reserved for patients with severe disease QTc<500 ms, with telemetry monitoring and serial QTc checks.
Regarding point #1, I suggest that these statements are true where a lockdown is not initiated until there is already a curve. But where a lockdown is implemented, along with other NPIs, as soon as the disease is detected in the country or community, then the goal would be to prevent the disease from taking hold in the first place. In this case, as dryam2000 pointed out, the lockdown wouldn’t need to be an extended situation, and the population could be protected from contracting the virus. The lockdowns need to be combined with closure of borders and airports in order to work. An internal lockdown could be lifted, while borders and airports remain closed, except for transport of essential goods, if necessary, until the danger of importing new cases has passed. Another reason lockdowns, which have been implemented late, have been less successful, is that not every household with sick individuals is able to isolate them from the others living in the house. This, combined with imperfect NPI measures inside the home, contributes to spread. I recall reading that the mayor of the South Korean city which experienced a large outbreak had asked citizens to also wear a mask inside their homes during that period. On the other hand, Sweden’s PM stated that the transmission there wasn’t as high as in some countries because a significant percent of the population lives alone. (Stockholm may be an exception – as in any large city, people live in closer proximity to each another.)
The discussion around herd immunity is quite interesting. One question in my mind is whether there is general agreement in the medical community that herd immunity is expected to happen, or has happened in some places with the SC2 virus, given its’ highly contagious nature and that it appears to have been lab manipulated? I’m also not clear as to whether immunity extends to a mutated strain. In other words, is herd immunity assumed to occur in the same way as with pathogens which have completely natural origins? Hopefully it is.
In any case, international and cross-border travel is now starting again. European countries have recently opened some borders, but only to countries where the coronavirus is under control. And 4 daily flights between China and the U.S. were scheduled to start soon. So we will see what happens….
We have a friend that is a psychologist and most of her clients are senior citizens. She tells me most all are terrified and will not leave their homes. Could it be that the fast learners in this aged demographic with the where-with-all to significantly isolate is the primary cause, or at least a major cause, in the lowered the death rate curve of present?
Anyone in the tribe that can execute a study that demonstrates the numbers of seniors with significant isolation capabilities that are hunkered down would add a priceless data point to the discussion.
This data would suggest that slow learning seniors or ones that can not significantly isolate (i.e. they have to live with a person in a younger demographic that has to go into the public space frequently) are the one’s showing up in the death statistics.
My gut tells me we are likely two pronged with the lower death rate; doctors learning the most effective treatments AND the fast learners in the aged risk group hunkering down.
This is all anecdotal without data, but a good questionnaire from the AARP data base could give some good indications as to the full set of real causes in the lower death rate of present.
C. Stone
Long term care facilities have also been a major source of transmission and deaths for the elderly, whether they are slow learners or fast learners. Once this was identified, there was a big push in many areas, to protect the residents of those facilities, and new protocols have been put in place. In general, any situation where people must live in close proximity to others and share common spaces such as dining rooms and bathrooms, are experiencing outbreaks. In many countries, nursing homes, prisons and migrant accommodations are at risk.
My sense is also that many people who are in high risk groups, including the elderly and also younger people with comorbidities, are trying to protect themselves by staying home if possible. This is combined with more knowledge in the medical community about how to treat the virus for those who are hospitalized. Also, some people have pointed out that in many countries the most vulnerable may have already been exposed. Let’s hope the death rates continue to go down!
Absolutely no mention of Zinc. It has been known for months that the key is Zinc.
Results would be much better with Zinc
Some senior citizens may be terrified to the point of cowering at home in self-imposed house arrest, but one has to ask what they are achieving. Living as long as possible is not a worthwhile ambition if one’s life consists of nothing but staring at four walls and watching network TV.
Living well as long as possible is much more sensible goal, even if it involves a risk of a shorter life. What is the point of living with no social interaction, no travel, no outdoor activities, no shopping?
Obviously, taking all of the prudent precautions of hand washing, mask wearing and avoiding mass gatherings of non-mask-wearing hordes is only common sense. But, even with those limits, life can still be not only worth living but actually fun and productive. We are all actors in a play with no rehearsal. We can give a great performance or skulk in the wings afraid to take part.
Once we get past the proverbial ‘three score years and ten’ we seniors are living on borrowed time. Sooner or later we are all going to die; most likely from heart disease, cancer or dementia. At our age, Covid-19 is not the most likely reason we will fall off our perch.
The more of that borrowed time we spend cowering at home the less we have to enjoy what short and rapidly diminishing period we have left.
Mohammed Mast and Sand Puppy.
After re-reading the Henry Ford Hospital Study this morning and noting no zinc was used, I started a literature search on Zinc and ionophores. This paper caught my eye. Back in 2010, Ralph S. Baric and other coronavirus researchers studied the potential for Zn and ionophores to block viral replication in vitro and in cell culture. That’s 10 years ago
https://pubmed.ncbi.nlm.nih.gov/21079686/
What first suprised me was how old these data are. We’ve known this for a long time. But then what caught my eye and startled me was the author list. Ralph Baric.
In 2015, Ralph S. Baric and his protege, Shi Zheng Li from Wuhan Institute of Virology, among others, published their creation of a chimeric SARS virus with S protein adapted for greater infectivity and morbidity - part of the gain of function research program:
https://www.nature.com/articles/nm.3985
Notice what they report:
“The results indicate that group 2b viruses encoding the SHC014 spike in a wild-type backbone can efficiently use multiple orthologs of the SARS receptor human angiotensin converting enzyme II (ACE2), replicate efficiently in primary human airway cells and achieve in vitro titers equivalent to epidemic strains of SARS-CoV. [original SARS]
Additionally, in vivo experiments demonstrate replication of the chimeric virus in mouse lung with notable pathogenesis.
Evaluation of available SARS-based immune-therapeutic and prophylactic modalities revealed poor efficacy; both monoclonal antibody and vaccine approaches failed to neutralize and protect from infection with CoVs using the novel spike protein.”
We synthetically re-derived an infectious full-length SHC014 recombinant virus and demonstrate robust viral replication both in vitro and in vivo. Our work suggests a potential risk of SARS-CoV re-emergence from viruses currently circulating in bat populations.
Now if Drs. Baric et al - who are world-renowned coronovirus experts - demonstrated the potential risk of SARS Cov re-emergence not responsive to immune therapy or potential vaccine therapy via "gain-of-function research, but also did research to show the potential for Zinc and ionophpores might be effective at inhibiting replication of RNA-viruses (of which SARS- COv-2 is one), then why - now that there HAS been a “re-emergence” of a SARS Cov virus - aren’t they vigorously advocating for post-exposure trials of cheap and available Zinc in combo with ionophores (of chloroquines and quercetin flavanoids are two examples) to mitigate this disease, if their own research shows this simple treatment has potential but immune modalities don’t?
I’m suffering cognitive and moral dissonance. I think I just went down the rabbit hole.
Erratum: The investigator’s name is Ralph S. Baric, not Robert Baric. My mistake and my apologies. You can see that author list on cited papers.
You are one helluva conspiracy theorist uh I mean realist.
Rabbit hole indeed
I could see why pharma would push more expensive alternatives, but what I’m having trouble processing is the academic researchers - the folks doing GOF research, ostensibly to help us confront pandemics, funded “we the people” - aren’t now aggressively advocating studies to demonstrate the clinical efficacy of potential readily available interventions they themselves reported.
Great points Boomer - I agree with you. On the other hand, anyone I know who is ‘hunkering down’ whether older or younger, sees it as being a short term thing, perhaps for several weeks, not for the rest of their life. I think they prefer to be ‘healthy and hunkered down’ rather than ‘sick and hunkered down’ or in the hospital. After it passes over they’ll go back to being active again. Of course, if ‘this pandemic thing’ as Jay Leno calls it, is here to stay, then at-risk people will probably accept that and make adjustments in their life. Everyone has a different view, different health situation and different values - and some are more risk adverse than others ![]()
Yes when one takes the Red Pill and delves deeper into the Matrix being stunned is a normal reaction.
US colleges and universities though lily white are far from pristine institutions. The ones established before the Civil War war were built by slaves or by money from the slave trade. That upstanding gentleman John Hancock himself, who was responsible for the Boston Tea party was a slave owner. Harvard, Yale, Brown, Columbia, UVA and others have deep connections to slavery. The rich contributed mightily to higher education and thus were able to control the narrative.
https://www.apmreports.org/episode/2017/09/04/shackled-legacy
J D Rockefeller got the ball rolling by giving millions to tada Johns Hopkins and Harvard for public health. At the same time he was bankrolling the fledgling pharma industry. He even gave money to China for the same reasons. It is naive to think that money came with no strings attached, whether explicit or implied. Virtually all agricultural research is funded by big ag. Do the name Monsanto mean anything to ya? Harvard was involved with the Sugar Association to produce research promoting sugar and downplaying its role in health issues. Articles were published in the New England Journal of Medicine. (are we stunned yet that they would publish negative articles about HCQ?)
Foundations have been funding chairs at colleges for a long time and wield enormous influence so as we have seen from the Lancet to NEJM money talks and the truth is not on the agenda.
Thanks for your research.

Someone in the community posted this. I think I’m at 3.5.