First, I want you to think closely about how the flu is spread, The flu is spread by surface not by close contact with infected person. How do we know this? Simple the flu season. The flu is much more prevalent during winter mos. Why? because temperature and humidity… affects survivable ? on what In vivo? or on surfaces? Yes, on surfaces.
This Covid has been demonstrated to survive up to 5-9 days on difference surfaces - that is much longer than 72 hours max of flu.
Also, bacteria is quantitative. You have to have a substantial load to get an infection. You only need one virus. So, I dont understand this load stuff… Sure the higher the load the more chances - but if you get just one virus in your eye or mouth - I do not see how you are not infected… I am not saying there are no front-line defenses ( SIgA ) that could potentially kill it. But I think its rare - I think anything above 1 virus will get you sick. I agree with the inoculation load and severity of illness. 1 takes time to reproduce to substantial counts vs - a huge load from someone coughing on your air. The low innoculum amount from a surface will just give your immune system a good 2-3 day head start. which could keep things from getting bad. You still are sick.
The Truth will come out.
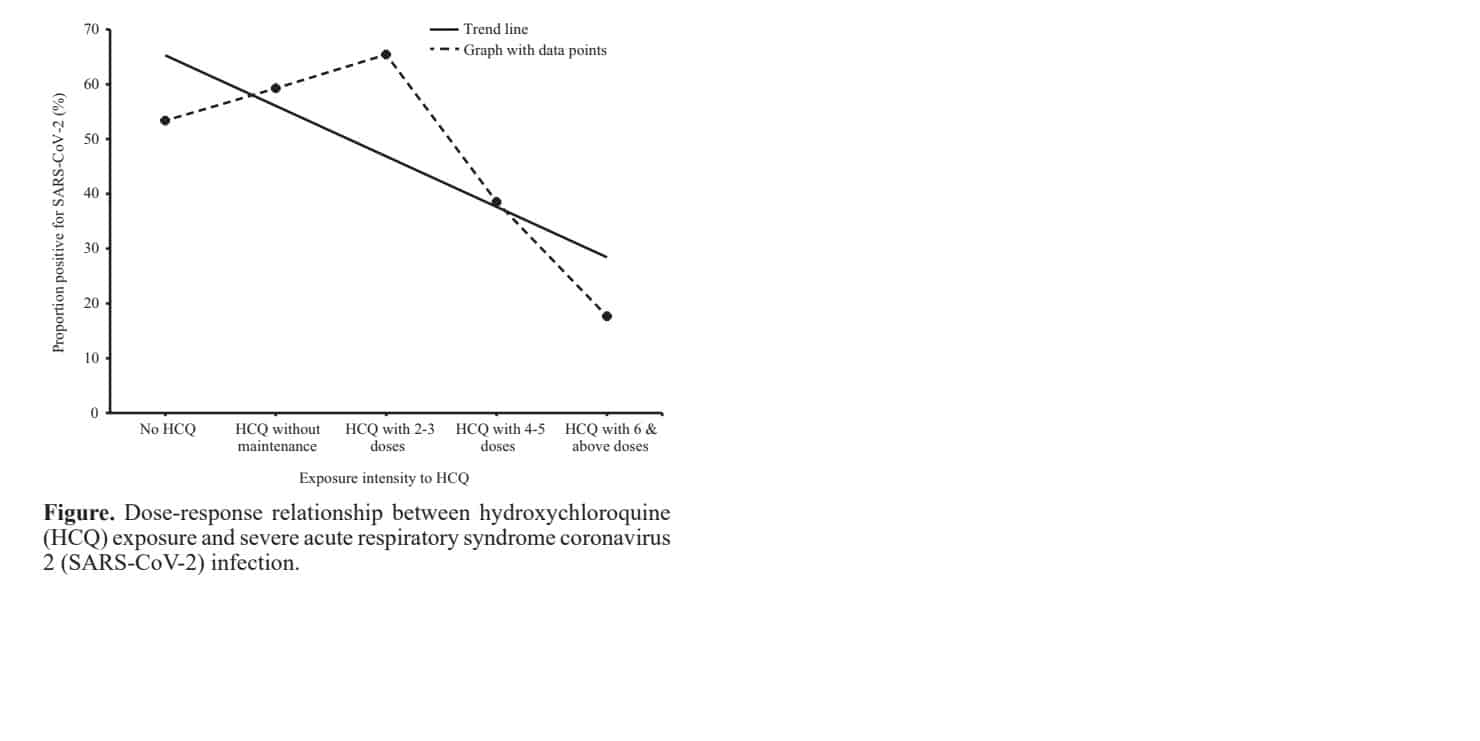
https://drive.google.com/file/d/1e26FOJfF4akP7-aMQjE_BGxTHBjrgo1e/view The pivotal finding of our study was the noteworthy benefits of HCQ prophylaxis. It was identified that simply initiating HCQ prophylaxis did not reduce the odds of acquiring SARS-CoV-2 infection among HCWs. However, with the intake of four or more maintenance doses of HCQ, the protective effect started emerging, and in the adjusted multivariate model, a significant reduction (>80%) in the odds of SARS-CoV-2 infection in the HCWs was identified with the intake of six or more doses of HCQ prophylaxis. This dose-response relationship (Figure) added strength to the study outcomes.For those visual learners;
Logically, I see option 2 as the only option. But in my heart know option one is the only option that will play out. But it just goes to show about human nature… as you say, the sheeple follow the psychopaths. Certainly wont find it the other way.
We would knock this sh&^& back. and allow us time to save the economy, our life-styles and time for a proper vaccine.
OTC may be a bridge too far… for now I would just like to see State and Federal entities getting out of the patient:Doctor relationship, as with any other prescription medication. The efforts being made against doctors and pharmacists in the case of HCQ are unprecedented, unwarranted, and amount to a death sentence for many Covid-19 sufferers. This is a crime against humanity and we need to expose it.
Abstract
Background & objectives: Healthcare workers (HCWs) are at an elevated risk of contracting COVID-19.
While intense occupational exposure associated with aerosol-generating procedures underlines the
necessity of using personal protective equipment (PPE) by HCWs, high-transmission efficiency of the
causative agent [severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)] could also lead to
infections beyond such settings. Hydroxychloroquine (HCQ), a repurposed antimalarial drug, was
empirically recommended as prophylaxis by the National COVID-19 Task Force in India to cover such
added risk. Against this background, the current investigation was carried out to identify the factors
associated with SARS-CoV-2 infection among HCWs in the country.
Methods: A case-control design was adopted and participants were randomly drawn from the
countrywide COVID-19 testing data portal maintained by the ICMR. The test results and contact details
of HCWs, diagnosed as positive (cases) or negative (controls) for SARS-CoV-2 using real-time reverse
transcription-polymerase chain reaction (qRT-PCR), were available from this database. A 20-item
brief-questionnaire elicited information on place of work, procedures conducted and use of PPE.
Results: Compared to controls, cases were slightly older (34.7 vs. 33.5 yr) and had more males
(58 vs. 50%). In multivariate analyses, HCWs performing endotracheal intubation had higher odds of
being SARS-CoV-2 infected [adjusted odds ratio (AOR): 4.33, 95% confidence interval (CI): 1.16-16.07].
Consumption of four or more maintenance doses of HCQ was associated with a significant decline in the
odds of getting infected (AOR: 0.44; 95% CI: 0.22-0.88); a dose-response relationship existed between
frequency of exposure to HCQ and such reductions (χ2
for trend=48.88; P<0.001). In addition, the use
of PPE was independently associated with the reduction in odds of getting infected with SARS-CoV-2.
J8ZnI7V7PsIndianJMedRes000-5413382_150213
If you can get 6 doses down, your chances of catching SC2 is cut by 80%. This, for frontline healthcare workers.
Likewise, “vitamins” seemed to help even more. AZI actually seemed to increase risk.
PPE: gloves and masks were also critical - a big reduction in infection, although not as large as taking HCQ.
Biggest activity risk factors: “Not wearing PPE”, conducting endotracheal intubation, as well as working in the ICU with suspected or confirmed cases on a ventilator.
Housekeeping staff had the largest risk, as well as “being male”.
And of course nobody died from taking HCQ. Side effects: not measurable (cases and controls had roughly similar instances of nausea, headaches, and diarrhoea).
It’s not an RCT, but - I can definitely see why India has told the WHO to get stuffed.
Based on this, if I were a frontline worker, I’d be sucking down HCQ + vitamins - and definitely making sure to wear my mask and gloves, especially if I were working in an ICU and/or conducting those endotracheal intubations.
Because - science!
This twitter thread, from a Doctor who has published using data from Africa and thus knows firsthand the difficulties in acquiring it, is yet another epic take down of the clearly fraudulent data behind the Lancet study. Read the whole thread of 15 tweets!
https://twitter.com/JNJarvis76/status/1267072918623866880
Here is a sampling;

Under 1000 cases, 10 fatalities? Nothing to see here, folks; move along.
I was visiting there a decade ago as an epidemic was developing, and they had the first fatalities in the W. Hemisphere, IIRC. So they’ve been on alert, and probably not shy to try cheap, available solutions, especially in a tropical climate.
Nothing like sitting two seats away from someone coughing on a plane to make you wish never to travel without masks in your carryon.
My contacts in CR cite HCQ being used in prevention, couldn’t find published confirmation of how when and where beyond what Chris has cited.
Costa Rica, along with other mildly-infected countries, might want to open up their tourist industries ASAP. But when will they want to allow US Americans?
A recent article in Tico Times (English) says HCQ is being withdrawn from use there. Pressure much?
“That’s a nice healthcare system you’ve got there. Be a shame if something was to happen to it.”
Might I suspect that around the world, medical careers, appointments, awards and conferences operate at a very politicized level?
The “NIH”, meaning “not invented here”, operates to prevent renegade solutions until, after an appropriate interval of forgetting, it can be discovered by “the right people.”
Just as mask-wearing can be rehabilitated – too late for tens of thousands of lives lost – when it is announced and promoted by the (same?) “right people.”
DJT gets something right for once, for himself obviously, and they choose that hill to die on? Stupidity all around.
Science is science. No such thing as half-science. Being half as dumb as your Fox-watching neighbors? Groupthink in an age of propaganda.
Education has declined, yes; but it was probably never strong enough to overcome this intense an effort at control from the top.
And to think, the country that landed men on the moon a half century ago can’t shut down a person-to-person pandemic transmission. Impressive!
Like washing your hands…except in your throat.
A new study published in the journal Function looked at the possibility of using commercially available mouthwash against COVID-19. According to a previous study, mouthwash – aka oral rinses – can destroy bacteria by disrupting and dissolving the lipid shell that surrounds them. Viruses, just like SARS-CoV-2 (which causes COVID-19), possess a similar lipid shell. So, gargling with mouthwash could potentially inactivate coronavirus in the throat, helping to reduce the spread from coughs and sneezes. https://nutritionandhealing.com/2020/06/01/covid-19-could-mouthwash/
Makes a ton of sense to me - again on the hygiene I spoke about earlier… But to educate people? How? Perhaps advertising by makers of mouthwash. with a price reduction because they will sell 8 times as much as normal.
If they are withdrawing HCQ. Its simply because the US wrote them a check…!!
The statement says the decision was based on new information ( US ) and recommendations from the WHO. ( US )
however, in the article and statement:
Costa Rica has used hydroxychloroquine in the past as a treatment for malaria, rheumatoid arthritis, and systemic lupus erythematosus. In those cases, the institution indicated that no serious side effects were generated.Utter political sh&^ show.
gloves and masks were also criticalI couldn't see what effect the gloves had and still don't understand the ways in which gloves might prevent infection, in either direction.
Thanks, Ision, for injecting Clint into this sagacious company. I actually considered that for a moment as my handle. Just an old dude with a bad attitude. ![]() No, not much different. Now I drink my beer with the deer in my backyard, better company than the barfly locals. Good moats make good neighbors.
No, not much different. Now I drink my beer with the deer in my backyard, better company than the barfly locals. Good moats make good neighbors.
“100,000 COVID-19 patients including about 15,000 treated with the antimalarials,”
This jumped out at me, as a question of whether even a number like 15,000 specifically verified CV19 patients would have been administered an as yet unapproved drug in a hospital setting, which these objectors are holding against, probably now with greater success, and yet claim has been tried so extensively.
Even worldwide; if known to be a preventive, then those countries would not have passed it into their hospitals, IMO. Why waste it? Were any of these really “studies”? Just not logical, at least at the scale they claim, or organized so quickly against such a recent virus?
Correct me if wrong, but my quick reading of the subject said they got their “data” from online searches of medical data sites, not (?) from individual hospitals. A few large “studies” might have gotten them numbers totaling close to 100,000 patients, but the inconsistencies between the study sources would disqualify any aggregation of wildly differing reports into one credible offering to the Lancet.
Oh the fun we used to have in Physics lab, fudging the inputs when we knew the desired results.
Remember, at first they were saying don’t get it because the lupus and other people will be deprived. Then the attacks really intensified. And they did protest too much, to my nonclinical mind. (Oh, and 3 out of 4 doctors in white lab coats recommend Marlboros. Really.)
But the 15,000 treated with HCQ in hospital to begin with just doesn’t sound plausible, whatever the timing of administration. Just an interpolation, an abstraction from a few numbers they wanted to believe?
Oh, and GET OFF MY LAWN! There, I’ve had my say for today ![]() (P.S. I’m feeling better now. And you will, too, Chris, if you’re ever feeling grumpy, you can shout it out across your huge new lawn, and no one will hear you!)
(P.S. I’m feeling better now. And you will, too, Chris, if you’re ever feeling grumpy, you can shout it out across your huge new lawn, and no one will hear you!)
(BTW, I think I’ve only been to the Ch. Gorge once, and I can’t remember if that’s where the skinny-dipping was; I know it was at the Green River in several places for sure, maybe at your old backyard? Imagine now wearing the mask, and little else… ![]() )
)
Thank you for this post. Masks are harmful and ineffective, i.e. we don’t have enough masks because we didn’t plan. HCQ is dangerous and ineffective, i.e. we don’t yet have enough supply for the military, medical field, first responders, and public at large. In the interim, agenda driven, false narratives, people die…and no one held accountable. Yes we should all be very pissed. This is criminal.
My experience as a long-term carer for my son was that the issue was hospital hand washing does terrible things to your hands. To maintain normal sanitation (before and after entering a room, before and after entering the toilet, before and after eating) required me as a visitor to wash at least 20 times a day. The doctors had it worst because they saw every patient on the ward and had to use it before and after each one. After a few months I started to develop cracked skin and dermatitis. Thankfully I got to go home before it progressed to the bleeding sores point. I don’t think normal gloving/degloving is as good as washing or sanitising since it’s so hard to do without contaminating the inside. However, it does save your hands and it’s necessary if you do have open sores due to the hand washing.
If wearing PPE, double gloving is necessary for proper doffing procedure in order to get a clean surface to manipulate things part way through. I suppose you theoretically could just wash your hands but there is the issue of fomite contamination of the paper drying towels and the skin issues if you do it a lot.
yagasjai - Thank you for posting these interesting articles. For me personally, this information doesn’t change my approach at all. Everything that comes into the house is still treated as if it is contaminated, as well as surfaces (and people) that we encounter outside the house, and we act accordingly…
Also, where we’re living, masks, hygiene measures and social distancing have been mandated by the government since the beginning of their cautious steps to re-open society, and this has worked out quite well so far. Masks are compulsory indoors in every open establishment, and are optional outdoors. The government has also been very good about communicating from the beginning, that the goal is to get, and keep, the Reproduction number at or below 1 to stop the exponential spread in number of cases, as well as to protect the ICU hospital units from becoming overwhelmed. So far they have been able to achieve this, and in fact the hospitals have been able to accommodate some Coronavirus patients from other countries as a result.
Last week I had a crown put on by my dentist. It had been delayed well over a month because of the Covid. They have a standard protocol that ALL patients gargle with mouthwash before being treated. Not sure what it was, but almost certainly contained hydrogen peroxide. Another simple, inexpensive, and likely effective means of reducing the spread.
Jim - the thread was quite interesting, and also the update he added afterwards with respect to the 437 African deaths in the original report (reference to Tweet 3):
Conclusion:
“Evidence on the benefits and harms of using hydroxychloroquine or chloroquine to treat COVID-19 is very weak and conflicting.”
Link here
https://www.acpjournals.org/doi/10.7326/M20-2496