It is OTC in many countries. But US medicine likes to set the bar high, with prescriptions (that doctors are threatened for giving) to pharmacists (explicit banning for off-label use in major chains) to ag supply stores (get written proof it is for animals).
Why such special sanctions against IVM? When drug companies tried and failed to produce vaccines against AIDS and Lyme disease, out of desperation people started experimenting with it (yes even the horse paste) and many reported success. Books were written and available on Amazon.
It is hard to find those stories anymore after massaging of the record by the Ministry of Truth. Ivermectin is really really dangerous to big pharma vaccine profits.
Next on the agenda is making supplements like C, NAC, D, flavenoids, zinc, melatonin prescription only.
Personally I don’t think they hate us. They just want the money.
Even more interesting how one person can hijack this whole thread under the guise of “discussion”, while there isn’t actually any room for discussion. Positions have been taken, allegations are being made, data and analysis is being ignored.
Yes, J, you are tiresome and sounding insincere. The body of work that Chris has published and presented, OVER TIME, is the sauce. You ignore at your peril.
If you don’t want to understand how and why Ivermectin works, that’s your problem, especially if you don’t want to put in the time and effort. Go ahead, trust big Pharma, and the health system. We see how they treat Covid patients.
”Oh, you have Covid? Go home and take Advil, and if your lips turn blue, give us a call, where we’ll fill you with useless Remdesivir and intubated you. Maybe you’ll live, maybe you won’t, but we still get paid”
Or, you can educate yourself, instead of complaining, and expecting to be spoon fed by others. Yeah, I’m harsh, but plenty of others here with more patience than myself, have given you very good advice, yet, you whine and snivel.
YMMV
If the vaccine is really so dangerous for an individual, why wouldn’t COVID be even worse for that same individual?
Point of entry. SARSCoV-2 enters through nasal mucosa and or ocular mucosa. Elicits immune system reaction via generation of T lymphocyte, plasma cells, Helper 1 and TH2, and even memory B cells. As to “vaccine”, this first line of defense is mute. Besides the significance as to point of entry, no virus’s I’m aware of contain PEG, 1,2-distearoyl-sn-glycero-3-phosphocholine and “other” non disclosed proprietary ingredients. The immunological response to these chemicals alone can have catastrophic effects. Now lets consider the vaccines mRNA genome which only partially resembles the original SAR Cov-2 spike genome. Modifications were made to prevent spike profusion away from the “injection site” and additional proteins were encoded to prevent the spikes from anchoring into cell receptors. This was an assurance given to us by the manufactures. The SALK institute and other publications beg to differ. Unintended adverse reactions?
Dave-
I agree. “Minimum energy for the hijackers.” I can’t always bring myself to do this, but this time I did all right. ![]() And I saved the link to Lawrie’s analysis, so there’s that too.
And I saved the link to Lawrie’s analysis, so there’s that too.
Again. Chris’s analysis is - no harm will be caused by ivermectin, and if there is a benefit (which is indicated by the meta analyses), then NOT using ivermectin is one of those crimes against humanity.
Can’t imagine why the serial-felon-drug companies and the captured “health” regulators would have a problem with a cheap off-patent drug that (unexpectedly) works to help solve the pandemic they’ve been waiting a lifetime to create-and-then-treat.
A Profound video. Thank you for posting.
A Thrall, you say, Dr McCullough? How does a human enthrall a planet? He doesn’t; he cannot.
Further evidence of Mantid infiltration. (Ref: Dr. David Jacobs et al Kindle, Narrated).
Know this. They are impotent against our Rage. Rage will break the Thrall.
Yep prostituting one’s self for the you-tube dollar. There was a time however when PP had more integrity. I’m afraid its just turning into yet another “prepper” site where the effort to print the written word has been displaced by a lazier and more boring aural rhetoric of um’s and ah’s.
I’m sure the establishment is feeling very proud of itself as yet another voice against the status-quo slides quietly into the pit of self-ostracism.
Some people think visually, some prefer the written word, some prefer haptic. I think visually. The best is a mix.
It’s all communication.
From https://www.drew.edu/stories/2021/09/09/drew-university-nobel-prize-winner-refutes-ivermectin-meme/
Dr. William Campbell, along with Satoshi Omura, won the 2015 Nobel Prize in Medicine for the discovery of ivermectin.
Recently, a false quote attributed to him circulated on social media, claiming that ivermectin ‘cures’ COVID19.
In response to that, Dr Campbell issued the following statement:
“I utterly despise and deny the remarks attributed to me on social media on September 8, 2021,” he wrote. “I reject both the substance and the tone of the remarks, and resent their presentation as a direct quotation. The tweet in question was not concerned with science. I am a biologist with no claim to expertise in the clinical evaluation of drugs against viral infections. Thus, I have not taken a stand in support of, or against, the efficacy of ivermectin against COVID-19.”To the very fair questions JoshuaGreen is asking, another important one to add is: Is it risky for this community have such confident support for ivermectin's effectiveness against COVID19 when the co-discoverer of the drug isn't standing in support of it himself?
Assume that the spike protein Is the disease and all becomes clear. (supported by studies on rats who were injected with the spike protein and not the virus. Proving that the virus is the Vector of the disease.)
Now why would you accept an injection that promotes the production of spike protein?
The conversation is really going off the deep end tonight. Chris has done the deep dive to prove it’s safe. We have known for over a year that it works;
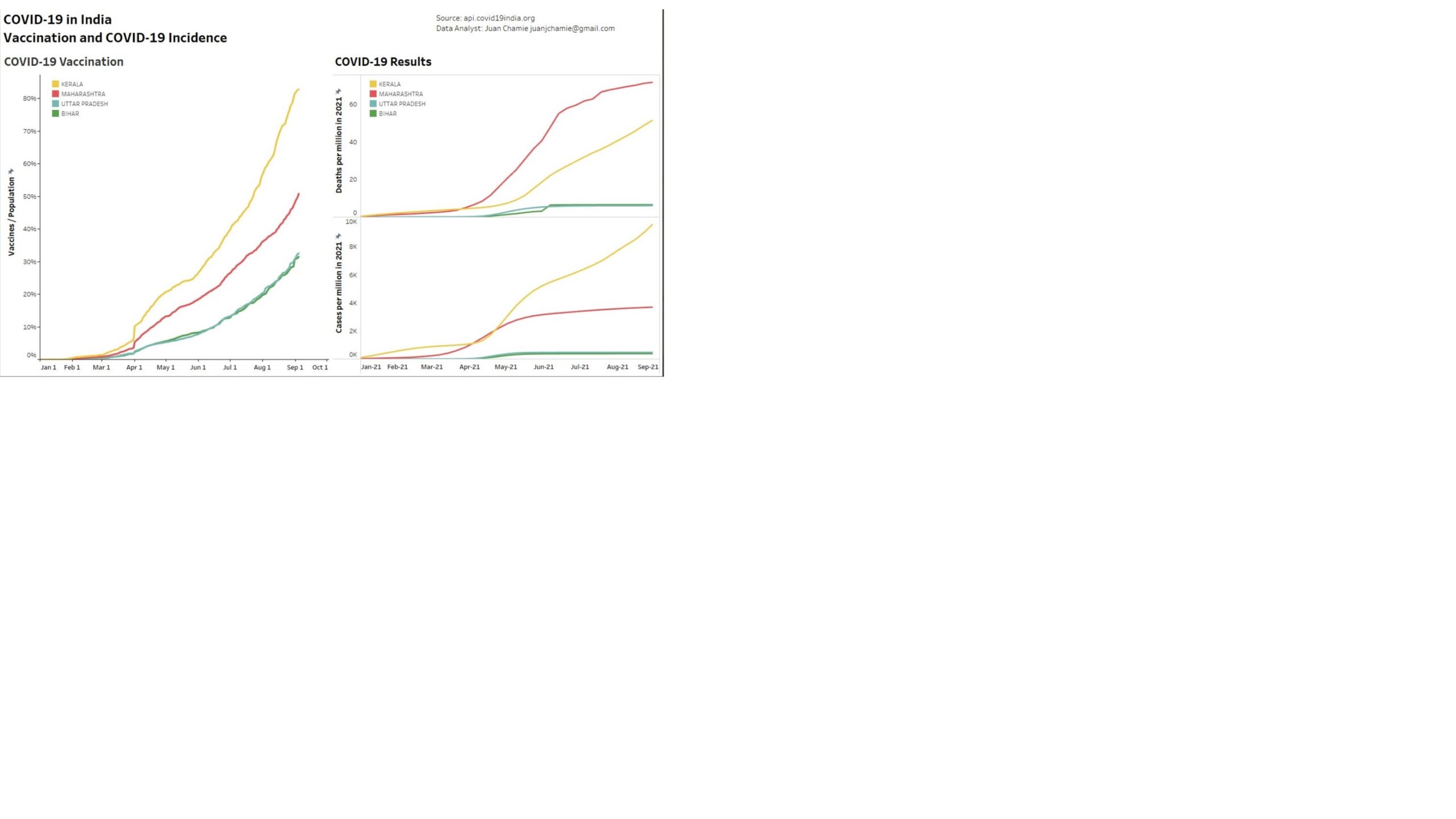
https://pubmed.ncbi.nlm.nih.gov/32251768/ Antiviral Res . 2020 Jun;178:104787. doi: 10.1016/j.antiviral.2020.104787. Epub 2020 Apr 3. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro Abstract Although several clinical trials are now underway to test possible therapies, the worldwide response to the COVID-19 outbreak has been largely limited to monitoring/containment. We report here that Ivermectin, an FDA-approved anti-parasitic previously shown to have broad-spectrum anti-viral activity in vitro, is an inhibitor of the causative virus (SARS-CoV-2), with a single addition to Vero-hSLAM cells 2 h post infection with SARS-CoV-2 able to effect ~5000-fold reduction in viral RNA at 48 h. Ivermectin therefore warrants further investigation for possible benefits in humans.So let's see if I can sum up the story; We have 40 years of safety data saying that Ivermectin is among the most safe drugs available. We have in-vitro data that says it shuts down viral RNA replication. We have loads of positive clinical data using cocktails based on Ivermectin and RCT's, almost all of which point to positive efficacy, many pointing to extraordinary efficacy. We have population level data within the country of India pointing out the stark contrast between the Ivermectin denying, heavily vaccinated Kerala and the much larger, lightly vaccinated Uttar Pradesh which has embraced early treatment and contact traced prophylaxis to THE NEAR ERADICATION of infection and death. You guys attacking Chris and attacking a molecule (Ivermectin) just seem silly.
Worse case IVM does nothing… It wont help you, wont harm you and doesnt cost but a few cents. No reason to not try.
Best case it helps, and still doesnt cost you or anyone much.
This one is a no brainer. But , what I dont get is why one doesnt not have a say in their own health care. I get people are not informed, but if they are asking or requesting - they should be allowed after weighing the risks with their care provider. I would take this even if someone told me it can kill me.
I’m just gonna point you guys to those two meta-analysis, and you can decide for yourselves. The drug is one of the safest ones out there, according to Chris-the-tox-guy. That’s the downside. Upside is - ivermectin might be a fantastic treatment for COVID19.
That’s the risk/benefit calculation. Some people have a hard time understanding risk/benefit. But I’m a trader; we have to be comfortable with risk/benefit at some gut level.
Here’s an example: If my assessment was that gold had a $2 downside, and a $0-$1000 upside, the trade would be an easy one to make. “A $1000 upside is awfully nice - worst case I lose two bucks.” I’d make that trade every single day. Eventually one of these trades will pay off big time, and I’ll be laughing all the way to the bank. [That’s called “sequenced multidrug therapy” in medicine-land]
Traders live in a world of uncertainty. We never, ever know if the trade will work out “for sure.” Everything is “odds” and “risk/benefit” and “making decisions in a state of uncertainty.”
I wonder what trader uptake of Ivermectin is?
I don’t even have too look at the odds on this one. You know it works. because how much they are trying to suppress it. The force is strong with this one. It could wipe out half dozen diseases , tomorrow. Ones that make huge money. things like depression ( which is a garbage basket catch all ) CFS, ( which is immune dysfunction as they have finally concluded ) as is gulf war syndrome, lupus, adhd, MS, and whole bunch of other autoimmune disorders. For all we know, and I firmly believe - this may be as effective , if not much more so, than all the drugs for HIV. ( at 300k per year / person ) They dont want the cheapo drugs… Somehow doctors and hospitals wont treat you because you didnt take vaccine( that hasnt completed trials ) for an illness that kills only old sick people mostly, but they will spend a truck load on someone with illness associated with negative and socially unacceptable or illegal behaviors.
This has never been about efficacy, this is about profitability. So applying your investment trade, I see no upside for the $$$ medical industry… Our health care is not determined by what is good for us , it is determined what is good for making money. so the trade in IVM - is a lose lose.
do you have a link to the video?
Chris, thanks for chiming in.
While I fundamentally disagree with the idea that an extremely safe drug with early positive observational signals has to have a bevy of RCT's before it can be used or recommended ...I think you're conflating two positions here. I don't know exactly why IVM was (I guess) by-prescription before COVID, but presumably those reason(s) are still in effect, so the question is really whether it's justified to ignore those reasons and make it, say, OTC now. Ignoring that question, I agree that it's perfectly fine for individuals to use IVM, as long as they take the appropriate version in appropriate doses. That doesn't mean that society has to recommend it as a treatment for COVID.
... I'm happy to discuss my reasons for believing it has a strong-enough positive signal to vigorously endorse and recommend.Which I'm happy to see you do.
I was unable to put any discussion of treatments on Youtube as even covering papers proved to be sufficient to get me banned. It happened twice. So I put my best efforts over here on the website and behind the paywall because I didn't want Google's prying eyes anywhere near my better work.I watched the previous video which got censored (before it was removed). Yeah, I agree that that removal was extreme, though you did note (in your follow-up) that you violated the terms-of-service by drawing a connection between the vaccines and reproductive health. So I kind of get your point, but when the discussion I'm interested in has been intentionally hidden and yet I'm repeatedly told (by commenters here) that I should be able to easily find it (without anyone actually providing a link), well, it doesn't do great things for the argument.
Back there you will find an excellent interview with Pierre Kory where he covers the totality of the evidence.Thanks; I'll check out what I can of those conversations, though it seems that some (but not all) of them are paywalled.
We have: 1) Powerful observational data from doctors who have collectively treated tens of thousands of early, mid and severe Covid patients with spectacular results. 2) We have country-level epidemiological data even including huge real-world experiments where a country (e.g. Peru) would go on IVM then off due to political pressures, then back on again with cases and deaths tracking with an ~1 week lag. See also Uttar Pradesh, Mexico City, parts of Brazil, etc. 3) Both RCT and prospective and retrospective clinical trials numbering in the dozens with the overwhelming majority of them showing very positive results. 4) Meta-analyses combining all the studies in 3 above showing exceptionally positive benefits. 5) My own anecdotal experiences which now number in the many dozens. Exactly zero of the people I have tracked closely through their use of IVM upon first symptom onset have progressed to the hospital. There was one member here (Steve) who reported not having that experience and going to the hospital despite IVM use. So including his experience then my results pretty closely track the studies that say "IVM is pretty darned good, but not perfect."Alas, the observational and epidemiological evidence can be confounded by numerous variables, and the RCTs and meta-analyses are currently coming under a lot of fire. This doesn't mean that there's no signal, just that it's hard for individuals to wade through all sides of this discussion. (As I noted in an earlier comment, it's something of a Gish gallop, with possibly strong claims mixed in with a lot of weaker ones.) I've seen you tear apart arguments that I've found persuasive, and I've seen others persuasively tear apart specific evidence for IVM efficacy, so I was hoping to see your critical take on the latter. At least in what I'd caught recently -- sorry, I find videos a rather awkward communication medium, and I don't catch all of them -- it seemed that you had been treating such claims with kid-gloves.
Well said.
I assume you’re referring to me. Please go back to my initial post (#9) as well as my quoting of Chris – something else which is difficult to do when information is presented via video – in #35. My only claims were that Chris’s decision matrix by itself isn’t reason enough to recommend IVM and that he didn’t discuss efficacy here or in his previous video. (Yes, I used the silly example of gummy bears in an apparently vain attempt to make my point. As a less snarky example, try replacing IVM with something like acupuncture in his decision matrix and then tell me which quadrant you disagree with.)
After that, there were several cycles of posts, similar to the following:
- Someone posts "Chris has covered the evidence in great detail."
- I ask "OK, where? I'd like to see that."
- They respond with "You should be able to search for yourself."
- I note that I tried searching and came up empty.
- They respond with "Here are a bunch of links at which IVM efficacy is demonstrated."
- I respond with "Yes, I can find those too, but I was interested in Chris's critical analysis of these claims."
- I'm told that searching is inherently hard on this site.
Josh is requiring that CHRIS explain this to him, rather than being satisfied with some other person presenting him the exact same evidence. For some reason, CHRIS had to be the delivery vehicle for the evidence. No bit of evidence that we lowly members could possibly provide - no matter how hard we tried - could possibly satisfy Josh.
It is clear that Josh isn’t actually interested in getting an evidentiary answer to his question. For some reason, it is critical to him that CHRIS be the information source, either in some recent video or presentation or personally or whatever.
Very curious. Never saw anything like this before. I wonder what’s really going on here?
Assume that the spike protein Is the disease and all becomes clear. (supported by studies on rats who were injected with the spike protein and not the virus. Proving that the virus is the Vector of the disease.) Now why would you accept an injection that promotes the production of spike protein?From a personal perspective I can offer two reasons:
- It seems likely that I'll eventually be exposed to COVID, and I expect fewer spike proteins from the vaccine than I do from a self-replicating virus.
- I know when I get the vaccine and can be on the lookout for (and ready to deal with) any side effects. (I can also time it so that unfortunate -- but not life-threatening -- effects will have minimal impact on my life.)