Useful chart. Would be good to see it for other countries. Anybody have that?

Ed Conway (@EdConwaySky) Tweeted: Here is the story of today’s @ONS mortality statistics in a single chart. The worst week for UK mortality (all causes) since records began.
The blue area shows the minimum and maximum mortality each week since 2010.
The red line shows you this year so far. https://t.co/j71W00tCVy
Sandman: thank you very much for this French research pre-print. This is not peer reviewed yet but seems very well written with a large sample number (84 given hydroxychloroquine and 97 not given).
I note that azithromycin apparently was not used.
The word “zinc” is completely missing from this paper.
I expect 24 hour wall to wall coverage of this paper by CNN.
Yeah, about those “negative results.”
A quick download of the PDF and then a keyword search returns this:

Isn’t that odd? Not only did they not use zinc, it was never even discussed to explain why they didn’t or how future studies might include it.
I equate this to running a critical test on the ability of a refrigerator to cool things but - so as not to confound the test - leaving it unplugged.
Wouldn’t you know it? Refrigerators are not effective at cooling things down!
Now why would these researchers not only leave zinc out but not even explain why? Or even mention it?
Whatever their motivations it wasn’t science that led the way. The ionophore qualities of HCQ are one of its key features. This is a known, established mechanism, as is the role of zinc in helping to fight viral RNA synthesis inside the cell.
Even if they didn’t want to include zinc on pass #1, they should have measured zinc levels in the blood of the subjects. Did they do this? Nope.
Again, why not? It’s data. Data is what you collect during a clinical trail. Certainly not every possible bit of data, but always the relevant parameters. Always.
I find this beyond weird opening up a line of thinking that it was an intentional exclusion of zinc. If/when it is later proven that zinc is an essential factor, and that this was well known prior to this “study” I sincerely hope the live-human testers involved in this publication face consequences for failing to obtain proper informed consent before running an experimental trial designed to fail.
Is that harsh? No. Why? Because zinc has both a very wide safety margin (including it wouldn’t have harmed anyone) and a known anti-viral role in combination with chloroquine. Patients should have been so informed and given a choice.
I am a critical care registered nurse with 40 years experience. It is clear you don’t understand DIC. It is the sequela in any hypoxic shock. CO2 is acidic and it is the PH change that triggers the clotting cascade . This is not unique to this disease and not caused by the virus attacking the blood. It is true that anticoagulation is the treatment upon onset, but PH control is the preventative. People should not take Asprin when they do not have coagulation pathology.
I’m getting a bit bemused by this. Surely we need studies with zinc and without it to test which is effective, so why knock this one?
Particularly since Dr Raoult, who has driven the debate in France, doesnt have zinc in his protocol.
This to me is one of the biggest indicators Of the politicisation: people saying on the one hand you must use zinc, but on the other hand touting Dr Raoult’s results, when he doesn’t.
We are now getting some documented studies coming through, and I’m dismayed to see Sandpuppy and Chris saying “nothing to see here”.
From memory, Raoult makes a big deal about starting treatment as early as possible.
“Everyone knows” you have to start in with the anti virals ASAP. That’s what they say with Tamiflu, right? Only useful if used within the first day. That’s stuck in my brain from somewhere. Google says: that’s been around since 2000.
Nutley, NJ -- September 18, 2000 Hoffmann-La Roche Inc. today announced new data on its influenza treatment Tamiflu™ (oseltamivir phosphate) that shows the drug’s benefits are significantly improved when taken earlier in the course of the disease. Tamiflu, taken within the first 12 hours of symptom onset, reduced the total duration of illness by greater than three days compared to treatment at 48 hours. The study data, entitled IMPACT, was released today at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC) in Toronto, Canada. https://www.gilead.com/news-and-press/press-room/press-releases/2000/9/new-tamiflu-data-shows-early-treatment-optimizes-benefit-for-flu-sufferersPresumably, if they wanted to do a real study to replicate or disprove Raoult's results, they'd actually give Raoult's treatment, and give it immediately upon receiving a positive test, and see how many got worse vs were cleared of the virus, just like he does.
No, the clotting cascade happens after hypoxia. Aspirin prior to becoming critically ill will not help. The proper Rx for hypercoagulability is Heparin.
What about warfarin?
I agree , this study would have failed, zinc or not. We know the doctors seeing efficacy are using it early. This would make sense with the zinc connection. Zinc reduces viral replication. So the action is to slow the replication long enough for the immune system to mount a defense. After all the cells are infected with virus, zinc or HQC wil do little or nothing. I think even the drs that believe in its use and efficacy will tell you it wont do jack for severe hospitalized patients.
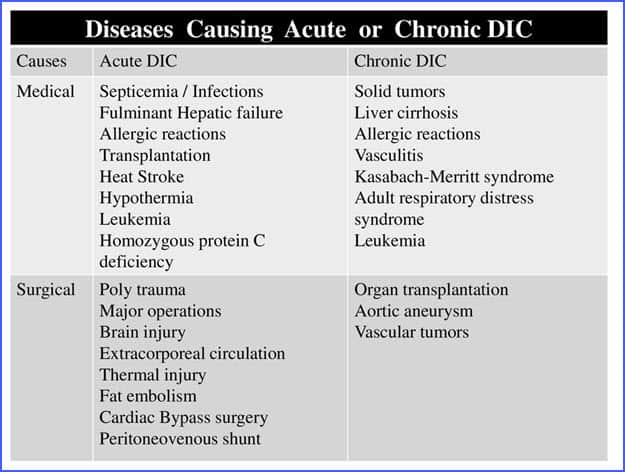
I am a critical care registered nurse with 40 years experience. It is clear you don’t understand DIC. It is the sequela in any hypoxic shock. CO2 is acidic and it is the PH change that triggers the clotting cascade . This is not unique to this disease and not caused by the virus attacking the blood. It is true that anticoagulation is the treatment upon onset, but PH control is the preventative.I'm sure you know a ton more about DIC that I ever will. However, when researching it, it seemed to me there were many possible causes and triggers. You are making the assumption that it is the hypoxic shock that triggers it. But what if it's the opposite? What if it's the coagulation that triggers the hypoxic shock? Can you rule that out? After all, it's not like DIC is triggered by any one thing:
 Seems to me like it's a very complicated cascade with multiple points where things can go bad.
Also, could you please reach out to the American Society of Hematology? As of yesterday (4/14) they weren't mentioning pH control in their recommended clinical anti-coagulation treatment guidelines.
https://www.hematology.org/covid-19/covid-19-and-coagulopathy
Sounds like they should know this...
As well, when I read through this extensive review of DIC and its clinical treatment, pH was not mentioned even once except as a set of clinical values for a patient case study (where the pH values for the doomed patient rose the entire time as they crashed over a ten day period).
https://academic.oup.com/ajcp/article/146/6/670/2703125
This came out in 2016 so perhaps it's outdated? Still, kind of surprising that pH isn't mentioned even once here either.
I try to do my research, but reading cannot ever come close to actual experience so thanks for weighing in.
Seems to me like it's a very complicated cascade with multiple points where things can go bad.
Also, could you please reach out to the American Society of Hematology? As of yesterday (4/14) they weren't mentioning pH control in their recommended clinical anti-coagulation treatment guidelines.
https://www.hematology.org/covid-19/covid-19-and-coagulopathy
Sounds like they should know this...
As well, when I read through this extensive review of DIC and its clinical treatment, pH was not mentioned even once except as a set of clinical values for a patient case study (where the pH values for the doomed patient rose the entire time as they crashed over a ten day period).
https://academic.oup.com/ajcp/article/146/6/670/2703125
This came out in 2016 so perhaps it's outdated? Still, kind of surprising that pH isn't mentioned even once here either.
I try to do my research, but reading cannot ever come close to actual experience so thanks for weighing in.
I am translating in post 7 from French to English - in the video he translates from the Italian doctor.
Effectively I know nothing about DIC, and subsequently cannot debate the points you raise. But as you speak from personal experience - I too know something about clotting as I have experienced a thrombosis experience - by having a heart attack. My experience has been that Big Pharma has lied about cholesterol to sell Billions of dollars worth of statins each year. Inflamation causing plaque to form in arteries - good dietary choices as a variable that can greatly improve your health - without statins. For me inflamation associated with blood clotting sounds familiar to me.
Again I am not a doctor, but from a logical point of view I would think that trama and the blood clotting to repair would be somewhat different than irritation causing inflamation and the breakdown of the cell structure. We are dealing with a virus that is a “foreign” invader - destructive at that.
Best wishes - please remember I am the messenger. The Italian doctor is the one that is talking about micro-thrombosis - which Chris amply talks about in this presentation.
@nordicjack
why describe the study as “failed”? It has given us a data point. From what folks are saying, it suggests that hydroxychloroquine given in this way (after significant onset, no zinc) doesn’t do much good.
If that pans out we have learned something useful about treatment, haven’t we? Of course we need many more studies.
It rankles with me to see Chris and others saying “show me the data” then the moment we get some data start saying “failure,” “nothing to see here,” and so on.
No, I would imagine it would not, your immune system has to do that. It does help zinc keep replication down while your immune system can do that. But that is just one action of the drug. There are others as chris mentioned regarding heme. That was the leading title by media… However the researches did note it did improve symptoms. and reduced inflammation according to biochemical markers. “what?” Hmm… and that was just a measly study of 150.
Interesting data about the 4 persons whose bodies they had autopsied: "The four decedents included male and female patients, ages 44-76. All were African American, and had a history of obesity class 2-3, and hypertension controlled by medication. Three of the patients had insulin-dependent type II diabetes, two had known chronic kidney disease (stages 2 and 3), and one was taking methotrexate.(this drug can cause blod clots and mess up your longs and suppresses the immune system, it seems according to drug info). On top of that there was “one decedent with prior partial lobectomy on the right side”. Also, all the patients received “antibiotic therapy throughout their hospital courses”. These also have side-effects that probably have weakened these patients even more.
Even the younger patients (>44) were suffering underlying diseases and probably for a while on prescription drugs: “We also note that two of our patients were younger than those commonly thought to be ask risk for death due to Covid-19, and without immunosuppressive therapy, though with obesity, hypertension, and diabetes - comorbidities often present in our patient population, and in the population of many cities with Covid-19 on the rise.”
Did they die from Sars-cov-2 or with Sars-cov-2 ? I’m not a virologist, but I wonder if one can even say they had Sars-cov-2 in their bodies, given that the RT-PCR test is not unquestioned and can deliver false positives…
The more I look at what is going on, the more I am astonished over the treatment of the treatments and standards of care.
First let me say that I’m not an anti vaxxer, in fact I currently work a company that aseptically fills parenteral drugs.
Why is it that the vaccine is the Gold Standard to all of these people, it doesn’t make sense. I know that it has been about 20 years since SARS-COV-1, but all those vaccines were basically crap since they caused more harm than good. Have we progressed that much with SARS vaccines or is this just a Hail Mary play.
You have countless doctors stating that the ventilator standard of care is most likely causing more damage, yet the standard of care must be followed for the almighty dollar to follow.
We have Subject Matter Experts questioning alternate therapies because they haven’t passed through the gold standard of the double blind study. Our Health Care Workers and others are at war, they should be able to adjust therapies within reason in the effort to save lives. This may require off label use of drugs, not following standard of care, etc.
Also if a vaccine is found to work, and be effective for the long term there is still a problem of scale. Lets say that in a best case scenario we only initially have to produce a vaccine for the 30% that don’t have herd immunity. So let’s guess that 2.25 Billion need to be vaccinated. This is of course assuming that the upstream bioreactors are available and scalable for the filling needs. This is also assuming that the all the consumables, materials and packaging can be made in quantities can be made in time. Whomever, gets the go ahead for the vaccine will need to have vendors produce things like vials, stoppers, and caps to supply to all of the various manufacturing sites.
These days the majority of vaccines are filled into vials with only the one dose in them (Single Dose vs. Multi Dose Vials). The best aseptic fillers these days run between 600-1000 vials a minute. Now, an aseptic line usually only does batch filling as opposed to continuous filling so there is down time to be had but we will eliminate this for our calculations, also automated inspection machine top out at about 600 vials per minute for cloudy solutions which the majority of vaccines are, labeling and packaging shouldn’t be a restraint. So we are limited with a throughput of 600 vials per minute or 36,000 per hour. So one line is capable filling the 2.25 Billion vials in 2,922 days. Now of course there are possibly many facilities around the world that are capable of this throughput. I personally think that the number of lines filling and inspecting at this rate around the world are on the low side, 30 tops. If we take that number it will take the worlds fastest 30 filling lines about 100 days to fill those 2.25 Billion vials. Of course the release and approval of the vials would most likely require some of the standard release requirements and take about 3 weeks per batch. Then you have distribution and supply chain times.
You say, well just have Ford, GM, Fiat Chrysler come and fill some of the vials. This would only be valid under the FDA, EMA, CFDA, and others really relaxing their rules. A new top of the line filler takes months to design and build, additional months to install and validate in an already validated pharmaceutical facility.
My point is that having a vaccine in quantity in 12 months is a pipe dream at best. We would be needing to identify facilities now, building more machines now, building bio-reactors now, deciding on packaging materials now.
If we are able to find that a cocktail like Hydroxychlorquine, Zn, and Azithromycin has benefit now regardless of not having a double blind study, we should be moving in that direction now since it will likely take 12-18 months to have the infrastructure and supplies to make a single vaccine in mass quantities and this will likely be at the expense of producing other vaccines and other injectable drug products.
These pills can be produced faster than vials (1000’s vs. 100’s a minute) and are already validated processes that are recognized by regulatory authorities.
Like I said I’m in the business and I don’t understand this odd infatuation by Dr. Fauci et. al. that we have to wait for a vaccine(s) that have yet to be confirmed with any human trials when we have mounting war time evidence of other treatments and standards of care that are working.
It’s like waiting around for a super-weapon that may or may not work when you have ingenious personnel that are cobbling together alternate solutions with the tools that they have and they appear to work but the “managers” refuse to see the merits and bide their time waiting for the super-weapon.
I follow a blogger from Italy who has been reporting on the local situation in Milan. She said that in light of the recent finding (blood clots), they are thinking of trying heparin as a treatment.
Hello.
I greatly appreciate the fine work Chris et al. have done in keeping us well informed on this topic. I have a healthy respect for the power of this virus and have been hunkered down for over a month now.
But I am having trouble reconciling Chris’s very scary overviews of just how dangerous and deadly Covid-19 is with the fact that the overwhelming majority of people who contract the disease suffer either mild symptoms or none at all. Couple that with the reports of tent hospitals being dismantled and predicted hot spots not materializing and I’m genuinely confused. Can anyone help me out here?
Thomas
Great update, but your updates make me want to overthrow the government. Screw the FED!!! Pitchforks and torches!!!
I think this stuff is half working. But feelings aside, this is a terrible example of what happens when it get’s into an elder care place.
https://www.wric.com/news/local-news/45-dead-in-coronavirus-outbreak-at-canterbury-rehabilitation-healthcare-center/
I just posted this… It will wipe out old people’s homes unlike the flu. https://www.wric.com/news/local-news/45-dead-in-coronavirus-outbreak-at-canterbury-rehabilitation-healthcare-center/
Having said that, it is a novel virus and I think we will all get it at some point. (Different viewpoint than Chris, lol.) Either viewpoint, it is always good to be prepared.
And if you prepare and nothing happens to you, then you are ready for your next hurricane-power outage-yellowstone-alien invasion.