@arterius2
“1/8 pregnant woman in NY giving birth test positive for Coronavirus, thoughts?“
You post a stat with no reference, no detail, and expect us to have an opinion on it. What is your opinion? What axe are you grinding? This is not really helpful to informed discussion.
Are you particularly surprised that 12.5% of young people in a virus hotspot have been exposed? A lot of this seems to be going on, trying to resurrect the “just like the flu” meme.
In April, 2.7% had been detected with antibodies, which, with a sensitivity of 70%, corresponds to 3.5% of those examined had already been infected with COVID-19.That's probably some very bad math right there. With a sensitivity of only 70% we have to assume (although it's not stated) that the specificity of the test is also less than perfect. If we even generously assume that the specificity is around 90% then the probability of seeing a detected 2.7% positive rate is pretty much 100% just due to false positives. If my recollection of testing probabilities is correct, even if the specificity was 97.3% you'd expect to record a 2.7% "positive" hit rate. Of course, those would be false positives. The only way the Dutch could record a 2.7% test sample result and then true it up to a higher number, as they did, would be to have a test that is 100% specific. It returns zero false positives allowing you to estimate some false negatives that you can toss on your pile of true positives. I am verrrrry doubtful of that being the case here with a test with a crappy 70% sensitivity.
There are a LOT more cases out there than show up in the “confirmed” case counts.It is undeniably true that there are MORE cases out there than show up in case counts. HOW many more is the $1,200 question. Thankfully, a family can live on that amount for up to ten weeks, according to Mnuchin. We all want to know the true incidence. We all want to know that people who do test for the SARS2 antibody (Ab) are actually now safe for life from reinfection by SARS2. That's probably not the case, sadly, but we can hope. It would be a mistake to use that handy table from the Salt Lake Tribune as definitive in any way. Why? Because of some pesky details that involve testing. Here we have to dive into the slightly complex world of test specificity and sensitivity.
In medical diagnosis, test sensitivity is the ability of a test to correctly identify those with the disease (true positive rate). Test specificity is the ability of the test to correctly identify those without the disease (true negative rate).To translate, if a test has a 90% sensitivity it has a 90% chance of properly delivering a true positive result and a 10% chance of delivering a false negative. If a test has 90% specificity, it has a 90% chance of properly detecting a true negative but a 10% chance of improperly registering a false positive. How do we make sense of this? Let's look at a real example. The FDA has approved Cellex's Ab test which has a sensitivity of 93.8% and a specificity of 95.6% Sounds pretty good right? Well, not so fast. In a population with an incidence of 100% those would be pretty solid. But something goes off the rails when the true incidence is low. Here's the math in visual form. Because of the interplay between the false positives and the false negatives, which involves some Bayesian math, the Sensitivity and false positive rate does not add up to 100%. So if that jumps out at you, just let it go. Let's begin with a true underlying incidence of 10%:
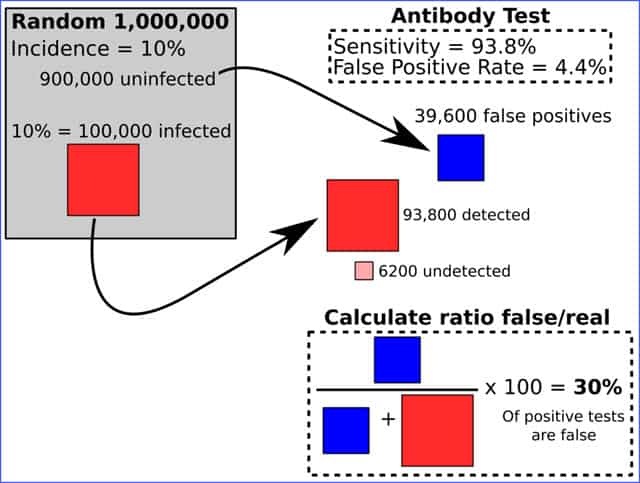 Wow. And Weird, right? If the true incidence is 10% in a population this test with it's 93.8%/95.6% stats is going to cough up a 30% false positive rate. So if you measured 10% as positive, the true rate would be just 7%.
But it gets worse as we nudge down the incidence curve. Here are the results for a 1% incidence rate:
Wow. And Weird, right? If the true incidence is 10% in a population this test with it's 93.8%/95.6% stats is going to cough up a 30% false positive rate. So if you measured 10% as positive, the true rate would be just 7%.
But it gets worse as we nudge down the incidence curve. Here are the results for a 1% incidence rate:
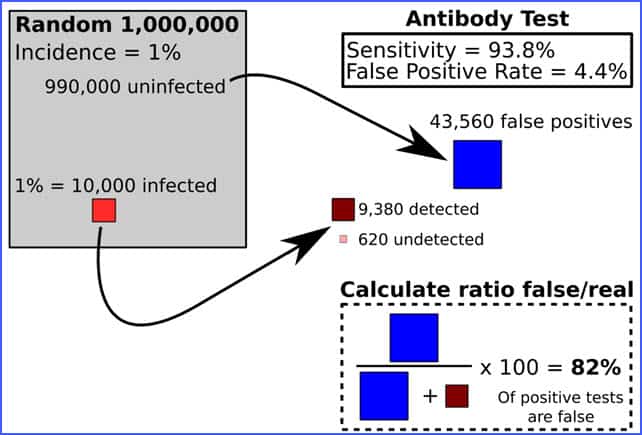 In a 1% true incidence population even the very good Celex test is coughing up 82% false positive test results. For every 100 positives, 82 of them actually weren't.
Many of the test results in the Salt Lake Tribune table were from earlier Ab test kits that weren't as 'good' as the Celex test. So, the summary is who the hell knows?
I wish we did.
Here's a very good article on the problem we face here:
In a 1% true incidence population even the very good Celex test is coughing up 82% false positive test results. For every 100 positives, 82 of them actually weren't.
Many of the test results in the Salt Lake Tribune table were from earlier Ab test kits that weren't as 'good' as the Celex test. So, the summary is who the hell knows?
I wish we did.
Here's a very good article on the problem we face here:
There are two key criteria we look for when we’re evaluating the accuracy of an antibody test. One is sensitivity, the ability to detect what it’s supposed to detect (in this case antibodies). The other is specificity, the ability to detect the particular antibodies it is looking for. Scanwell’s chief medical officer, Jack Jeng, says clinical trials in China showed that the Innovita test achieved 87.3% sensitivity and 100% specificity (these results are unpublished). That means it will not target the wrong kind of antibodies and won’t deliver any false positives (people incorrectly deemed immune), but it will not be able to tag any antibodies in 12.7% of all the samples it analyzes—those samples would come up as false negatives (people incorrectly deemed not immune). By comparison, Cellex, which is the first company to get a rapid covid-19 antibody test approved by the FDA, has a sensitivity of 93.8% and a specificity of 95.6%. Others are also trumpeting their own tests’ vital stats. Jacky Zhang, chairman and CEO of Beroni Group, says his company’s antibody test has a sensitivity of 88.57% and a specificity of 100%, for example. Allan Barbieri of Biomerica says his company’s test is over 90% sensitive. The Mayo Clinic is making available its own covid-19 serological test to look for IgG antibodies, which Elitza Theel, the clinic’s director of clinical microbiology, says has 95% specificity. The specificity and sensitivity rates work a bit like opposing dials. Increased sensitivity can reduce specificity by a bit, because the test is better able to react with any antibodies in the sample, even ones you aren’t trying to look for. Increasing specificity can lower sensitivity, because the slightest differences in the molecular structure of the antibodies (which is normal) could prevent the test from finding those targets. “It really depends on what your purpose is,” says Robert Garry, a virologist at Tulane University. Sensitivity and specificity rates of 95% or higher, he says, are considered a high benchmark, but those numbers are difficult to hit; 90% is considered clinically useful, and 80 to 85% is epidemiologically useful. Higher rates are difficult to achieve for home testing kits. But the truth is, a test that is 95% accurate isn’t much use at all. Even the smallest errors can blow up over a large population. Let’s say coronavirus has infected 5% of the population. If you test a million people at random, you ought to find 50,000 positive results and 950,000 negative results. But if the test is 95% sensitive and specific, it will correctly identify only 47,500 positive results and 902,500 negative results. That leaves 50,000 people who have a false result. That’s 2,500 people who are actually positive—immune—but are not getting an immunity passport and must stay home. That’s bad enough. But even worse is that a whopping 47,500 people who are actually negative—not immune—could incorrectly test positive. Half of the 95,000 people who are told they are immune and free to go about their business might never have been infected yet. Because we don’t know what the real infection rate is—1%, 3%, 5%, etc.—we don’t know how to truly predict what proportion of the immunity passports would be issued incorrectly. The lower the infection rate, the more devastating the effects of the antibody tests’ inaccuracies. The higher the infection rate, the more confident we can be that a positive result is real. (Source - Technology Review)
and a 14 percent rate of infection is a real s**t storm. I haven’t gotten ill yet that I know of, know plenty who have. Things like relentless 2 week fever with encephalitis symptoms, severe hypoxia (treated at home, bedridden for a month), etc…these are some who don’t get counted. I hope our attack rate is at least 50 percent by now, going through this a second time is too much to imagine and hopefully not coming to a town near you.
Wishing you a full recovery. Hoping this asymptomtic syndrome notion is true. TAke good care.
Saw this link in a comments section: https://www.nature.com/articles/s41423-020-0424-9.pdf and I’m pretty sure you have covered this recently.
The person who posted this link characterized the virus as airborne HIV. Is this accurate?
…and acute respiratory distress syndrome
http://www.pathologyoutlines.com/topic/lungnontumordiffusealveolardamage.html
The easy fix for “false positive” is to test twice.
In other cases where you test positive for something, you end up getting a second test, just to be sure. Pregnancy, HIV, cancer, etc. If you come up positive - you automatically get a second test.
While I don’t have evidence that’s what they did in this instance, I think it’s a strong likelihood that - given how that’s how things work in every other instance I’m familiar with, when the situation is relatively serious - it is likely true here too.
“Whoa, a positive test! Let’s do it once more so we are sure.”
So, if I’m right, then we can use that table.
My father reacted to the flu vaccine my parents got every fall at the mall with paralysis, but my mother reacted by losing her sense of smell and taste and then was diagnosed with Alzheimer’s. It is common for Alzheimer’s to have this effect, so yes, chemical nerve damage.
Since the CV numbers of cases are still going up and it often takes many weeks to recover (ten Diamond Princess patients are still in critical condition), the ratio of recovered to deaths is not an accurate measure at this time, as most cases are still in the limbo of “active:” while they could go either way, most will recover. The number of active cases not yet called is huge, and true CFR is impossible to determine at this time. That being said, SARS started with a low CFR but eventually went up to almost 10%, maybe because patients got an increased viral burden as it became more common in the environment.
This was a great presentation, thank you for all your thoughtful coverage of this topic. I am a practicing forensic pathologist in one of the hot zones in the USA. Regarding fibrin microthrombi in the lungs - I think this may just be a well-known feature of diffuse alveolar damage in general of any etiology, rather than a thrombotic (micro)angiopathy per se, but it’s too early to know for sure either way. I have seen and heard about some cases of systemic thromboemboli outside the lungs and in cases where Covid-19 was highly suspected, but PCR tested negative (possibly false negatives). It could well be that thromboembolic complications are a feature of Covid-19, and it would be very helpful to know that.
At least according to my observations, I also wonder why the greatest risk factor for severe Covid-19 disease or death seems to be obesity, which is possibly an even greater risk factor than age. Could it be increased ACE2 expression in fat, either in adipocytes themselves or supporting cell types? Or might it be decreased physiologic reserves in terms of heart and lung function that have to support a large quantity of body tissues (i.e. fat)? Or something else altogether? I don’t know the answers, and hopefully we will find them someday.
On another note, I am somewhat less optimistic than you in expecting a positive outcome for our country in this crisis, and what is continuing to unfold. Too bad we don’t have more informed and thoughtful people like you in leadership positions. As you are fond of saying, it didn’t have to be this way.
Not sure if this was mentioned previously, so let me apologize upfront if it was, as there are many posts on this site. It seems we are lost on how to handle this virus. How many cases are there? What is the fatality rate? How do we stop the spread without destroying the economy? etc. The solution is we test everyone! We test to determine if you have the virus AND if you had the virus! This should be our priority. If most of the spread is from those who show no symptoms then we will never get rid of this disease. If we do not know the fatality rate, then we will never know how serious this virus is. So we test everyone, maybe monthly if need be, or until we have enough information on this virus to determine a better action plan. I also agree with Chris’s comments on masks, and social distancing, etc.
I am only going to guess here based on my understanding of biology. The BCG vaccine is actually a vaccine for a specific bacteria that causes TB. Vaccines that target bacteria act differently than viral vaccines. I would say that somewhere in the vaccines response it trains the immune system to target pathogens on surface of the lungs. Something that is not innate to the immune system. These vaccinated people may have a slightly more trained response inwhich the immune system is already programmed how to deploy immune cells to the target location.
For those who don’t read French, just a quick summary from memory: The article confirms what Chris was talking about today. There is this micro thrombosis going on and it is to do with inflammation. In Italy this seems to be understood now and patients are now being treated with anti-inflammatory medication and this is having great results. In the US by contrast, the study says, the older protocol of avoiding anti-inflammatory treatment was leading to the current bad statistics. The study suggests we don’t need any quaranteen, just the correct treatment.
And that means the true mortality is low. The Danish data (cited above) actually comes from people who DONATED BLOOD and the blood was tested. This showed that true cases in that area were up to 70 TIMES the recorded cases. And the NY “Pregnant” findings (cited in the video above) showed that probably one million NY City residents had already been infected (one week ago). More and more of these numbers will come out.
Test everyone. No way. As soon as you give the government the rights to your body your their complete slave forever!
“Those who would give up essential liberty to purchase a little temporary safety, deserve neither liberty nor safety.”
Benjamin Franklin
If you are afraid of the virus - stay home! Many of us are not willing to give away the rights to our body so you can feel secure. I must say because I work with people I knew I would be exposed and I was. Got through it just fine and am in my 60’s. Now I see a whole lot of people living in fear. I suspect sooner or later most everyone will be exposed, just like the common cold. Soon the quarantine and virus may be the least of your problems?
AKGrannyWGrit
A little off topic but one of my pet peeves is inaccurate quotes. i am sorry nothing personal but there is no evidence ol Ben ever said that.
Just as Jefferson said that thing about inflation and deflation.
On the other hand I do agree with the sentiment
https://holistichealth.one/treatment-for-coronavirus/ Blessed are those helping others through this. The best thing is focus on the positive and what you can do. Instead of focusing on the “pandemic” ask yourself “what can I do to be best prepared for it.” Since I’m into holistic health and wellness I have a list of natural things anyone can do to be as safe from this outbreak as possible. #coronavirus #covid-19 #immune
Looks a lot like a european variant Covid-19-cytokine storm related death …anybody know if the hospital staff was tested or infected?
https://www.wlox.com/2019/12/27/espn-reporters-death-prompts-questions-about-dangers-pneumonia/