If in fact they are performing 125 exponential amplifications the multiplication factor is somewhere similar to the number of miles to the sun. My pet rock would test positive.
So I guess this discussion is focused on PCR testing. What about the other types of COVID-19 testing. Is their accuracy in question? Aloha, Steve.
well for your safety, I hope you’re setting a policy that all inside pet rocks must wear a mask or else they’ll get tossed out!
I used to run a Pathogen Dx microbial PCR screening test in a lab I worked in which I am assuming is similar to the detection methodology used with covid testing.
With PDx, the cycles were ran from a microarray with around 90 wells in a programmable thermo-cycler. After the cycles (which were also 40), small volumes of the cycled samples were placed on a glass plate and then allowed to “hybridize”, aspirated, then placed in a detector which took images of the plate (about the size of a microscope slide, a bit larger). I looked for info on what the detector did, but cannot find any from a casual search. More than likely, it operated off of UV or IR detection which should be noted that it probably was not a quantitative measurement (we had issues with the quantitative aspect of this tech).
So to answer your question making the assumption that covid test detection is similar to PDx: No, there is no way to know at which CT your sample had a positive result.
In order to do this, they would have to cycle your sample in multiple microarray plates which had defined CT to stop cycling, do post-cycle processing, then run in the detector for each CT cut off. I could be horribly wrong too.
I doubt they have the time to do this seeing as the volume of testing has only been increasing as time goes on.
Absolutely,
no tests, no numbers = no restrictions on constitutional rights and abhorrent gutting of our local economies…
I refuse both the test AND the vaccine… look at who is behind both the creation of this mess and the solution. Follow the money.
Where have we seen the strategy of controlled opposition before?..
Dr. Martenson, once again, the leading edge of common sense!
I missed your September video, but saw the one last night. Great minds think alike as I have been revisiting the credibility of the tests and going down rabbit holes.
If the tests are garbage, the whole narrative has no stable footing. This is besides the fact that the only attempt at investigating the origin of sars-cov-2 has been from compromised science hacks that obviously have vested interests in the zoonotic origin theory. Why are we a year into this and still no reasonable audits of BSL3-4 labs not only linked to the WIV, but worldwide? China now says that the virus originated in Italy. I had no idea, first off, that pangolins and bats hung out in the same caves, but that they also reside in Italy and have dual citizenship. Maybe that’s where they migrate to for the winter, eh? Very interesting symbiotic relationship there as the bats might be flying the pangolins over there?
Anyhow, a few points that were not addressed in the recent video:
(in no way a criticism or complaint, just wanted to add these)
1) EUA authorization was awarded to test kits which did not include human genetic material for potential false positives. This creates a problem which I will mention below. To make matters worse, there was no process of cross-lab or third party validation of said tests. From what I understand, the labs that manufacture the tests provided their own validation data to prove effectiveness and be awarded EUA.
2) There is no requirement for a negative control in any covid tests under EUA. This is what had initially stalled the roll out of the CDC test. So the scientists in all their great wisdom just chose to throw out the faulty component rather than solve the problem and provide a legitimate test by including both positive and negative controls.
3) Looking in detail at the CDC tests, the forward and reverse primers match exactly to certain sequences found in human chromosomes (I used ncbi blast tool). This ties into number one on this list. We know that these tests are not quantitative, but qualitative. What I do not know at this point is if there is any sorting of amplified genetic material such as gel electrophoresis (which they do not have time to do for the magnitude of tests being processed daily). If the detection methodology does not differentiate between say 500bp segments and 20bp segments, the amplified sample could contain any number of genetic material that the primers had an affinity to. This is a HUGE problem.
4) Technician handling error: Some components need to be stored at -80C in order for the test to work properly. These types of freezers are very expensive and hopefully all labs processing tests have these on-hand. If not, then the results are meaningless. As I mentioned in a reply to another comment here, I used to work in a lab that ran pcr tests to detect STEC and other microbes. We did not have a -80C freezer and the tests rarely produced usable results until we obtained proper cold storage.
EDIT: forgot one…
5) The RNA segment that is screened for with the pcr test is the nucleocapsid rather than S proteins or the famously unique segment of PRRA. I get that the S region is subject to greater selectivity/mutation, but miraculously, it seems to not have changed much although it has passed through millions of humans at this point. Regardless, the nucleocapsid may not mutate as much, but it is a very generalized segment that I am nearly positive is shared among other betacoronaviruses. Their choice of RNA segment seems very poor and I have yet to find an explanation of why they chose this. As we all know by now, the PRRA segment would be ideal to screen for Sars-cov-2 as it is not found in any similar betacoronaviruses.
Just a few things I wanted to mention to you. Hope you get a chance to read this.
---------- Forwarded message ---------
From: Long, Robert (Maine CDC)
Date: Wed, Dec 2, 2020 at 2:25 PM
Subject: RE: Positive Covid Test? Please Ask this Question
Good afternoon,
There has been a lot of hypothesizing about cycle thresholds for COVID-19 PCR testing. Here is the latest U.S. CDC information on the topic:
https://www.cdc.gov/coronavirus/2019-ncov/lab/faqs.html
Manufacturers of the tests approved by the FDA set the cycle threshold of less than or equal to 45. Maine CDC’s lab does not have authorization to alter that setting, as it is designed to create a peer-reviewed uniform national standard.
Respectfully,
Robert Long
Maine CDC
Comment: Seems like the test is of no value as PCR will find COVID-19 Dead or Alive.
I’ll continue with boosting my immune system (a la CM), and wear mask when in public places. -Bob
-Bob
Not that it makes me feel better about the situation, but at least I feel like I understand whats at play:
- In various “Third World” countries, lockdowns and businesses limited to 25% occupancy would rapidly lead to a substantial number of people starving in short order.
- In those countries where the leaders realized they are best served by a situation of “non-starving”, cheap medications are investigated and used to treat patients and life is kept as normal as possible otherwise because this is what the key supporters of those in power need most.
- In other countries, the lockdowns and small business carnage are seen as an acceptable price to pay while key supporters line up solutions that are lucrative for them or the shutdowns/lockdowns are seen as being valuable in their own right for some other reason.
If you are here you are probably in one of the countries handling things poorly but you are also blessed because you can take matters into your own hands as far as getting those well proven cheap treatments.
Being “on your own” isnt as bad when there are others around to help you
I had a couple links I wanted to share. The first one is a decent (IMO) primer, relatively non-technical, about test types (immunoassay vs PCR), accuracy, and collecting samples. Although Chris has explained “test accuracy” in the past, you may find the explanation here a good refresher on the details of sensitivity and specificity.
https://heavy.com/news/2020/05/covid19-coronavirus-tests-accurate/
The second link [indicates last update was July 2020] has some interesting evaluation data on tests by manufacturer. Among other information you’ll see are accuracy numbers, average CT, and one that I found most interesting, “supplier recommended CT cut-off”. In addition to a numeric entry like “<=40” you’ll see “None; any signal can be considered positive”.
https://www.finddx.org/covid-19/sarscov2-eval-molecular/molecular-eval-results/
For extra credit:
https://spectrum.ieee.org/the-human-os/biomedical/diagnostics/testing-tests-which-covid19-tests-are-most-accurate
http://www3.weforum.org/docs/FOP_Readiness_Report_2018.pdf
Please see the above link for a big report from WEF as to which countries are more “ready” for the GREAT RESET.
One hundred countries are profiled in great detail.
Also I look at the jobs advertised in the WEF and UN.
So those are two sources which can help decipher things.
From the jobs being advertized by the WEF, the are massaging government and business leaders in Japan and they are moving into India also by the looks of things.
From the Pilgrims Society, seems like UK in the lead, with commonwealthers of Canada, New Zealand, Australia, Jamaica and India also in the first string…
I need to analyze the UN jobs more as there are many but they seem interesting Civil Unrest alot…
Hospitalisations is also a major driver of policy on COVID-19. On current trends, US ICU beds will be 100% occupied by Christmas. I guess the non-ICU capacity would also be under strain.
My home province just formally asked the Feds and Red Cross for help building field hospitals.
Also some mysterious Apple Flavored Paste showed up in the mail today. Think Ill hold onto that…
On current trends, US ICU beds will be 100% occupied by Christmas.I tried to find a source for that. Couldn't. One place ICU bed utilization is tracked is at Healthdata.gov (here: https://healthdata.gov/dataset/covid-19-estimated-patient-impact-and-hospital-capacity-state/resource/82e733c6-7baa-4c65#{view-graph:{graphOptions:{hooks:{processOffset:{},bindEvents:{}}}},graphOptions:{hooks:{processOffset:{},bindEvents:{}}}}) Sloppy URL, I know. It is what it is. At any rate, when I download their data and then graph it I get this:
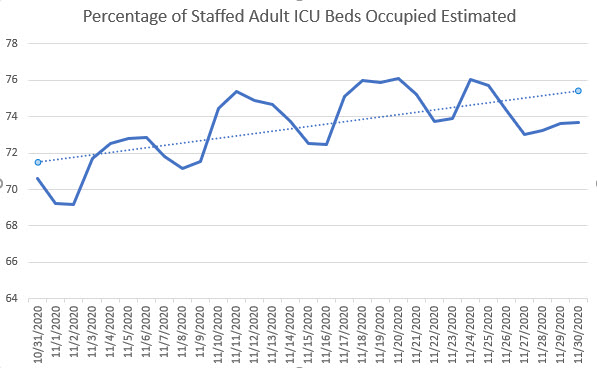 We could observe a slightly rising trend line. Or we could note that ICU bed CapUte is more than 2 full points lower than a few weeks back.
Either way, I can't get to 100% by XMAS.
Of course, this is all states. Individual states and locations may have issues, and I'm certain some do.
But I should also note that the historical CapUte is usually between 70% and 80%, as it should be in a for-profit business model.
We could observe a slightly rising trend line. Or we could note that ICU bed CapUte is more than 2 full points lower than a few weeks back.
Either way, I can't get to 100% by XMAS.
Of course, this is all states. Individual states and locations may have issues, and I'm certain some do.
But I should also note that the historical CapUte is usually between 70% and 80%, as it should be in a for-profit business model.
Comment on Belgium, A government list of directives is preserved from the Spanish Flu. # 8 Said to gargle several times daily with bicarbonate water. https://www.brusselstimes.com/belgium/103592/how-do-belgiums-coronavirus-and-spanish-flu-measures-compare/. This was very common. The use of baking soda in water was frequently declared as an effective preventative and treatment.
bit.ly/acureforgottenfb
Well here is a tale for the ages.
I am bullet proof to Covid. I have an arsenal of HCQ, Zpack, Ivermectin, and Doxycycline.
My Vit D level is 95. . My protocol is Vit D, zinc, quercitin, elderberry, selenium, copper, Nac, Vit C, and a ton of other supps.
If anyone thinks that will protect you from Staph I am here to disabuse you of that notion. I have never had Staph in my life till this year(north of 70) I have had it 4 (FOUR) times. I have been on antibiotics more than I have been off of them since February. It is nasty shit.
For the last four weeks I have been on Minocycline. My Dermo finally did a culture. I found out the AB’s I have been on were ineffective against Staph. So he switched me to Minocycline. That is some nasty shit. I dipped into the side effects and I had most of them. Nausea, Dizziness, Lightheadedness, Then I dove a lot deeper. Night sweats. 4 weeks of night sweats. So I talk to the Dermo he cuts the dose from 2 a day to one. Now for 6 days I wake up with a temp of 95-95. At 1pm it starts to go up to over 100 sometimes 101+ So Monday I call my PCP for a Covid test. I get both the PCR and the rapid. Rapid comes back negative. After 4 days of symptoms that is conclusive. He takes blood. I ask him what’s with the night sweats. He says probably hormone imbalance. So we do the thyroid panel.
This morning results of blood test are , thyroid normal but liver enzymes elevated. That is serious shit. So I ask well what do I do. The woman says I don’t know let me ask him. She calls me back and say come back in 6 weeks. lol elevated liver enzymes and come back in 6 weeks. So I ask well what do I have . She calls me back and say “what pharmacy do you want your prescription filled at”? I say “what for ? " She says “zpack” Lol thanks to Sunil I have an entire box of Azithromycin, HCQ< Ivermectin and Doxycycline. So I say well what do i have. She says I will ask him. She calls me back and says " he says you “probably” have Covid”. Now this is 2 days after having a negative test. So I say thanks and hang up. I get a call a little while later and It is the Dr.'s office. They have the results of the PCR. It is negative. Now the funny part is on Monday I asked two of the nurses what the CT value of the test is. They looked ar me as if I just landed from a spaceship from Mars. They had no idea what I was talking about . So I explained it to them. It reminded me of going into banks and asking if they knew how money was created. Same blank looks or " Yeah the government prints it"
So here I am having fevers for 6 straight days, night sweats for 4 weeks, elevated liver enzymes and I have to be the one to ask so what do I have and what do i do? So she says “I’ll ask him” She calls me back and says “If you don’t feel better by Monday come in to see him.” ROTFLMAO
Fortunately my wife knows an infectious disease specialist so she texted him and he agreed to see me. I have to get all my records together and sent to him. The PA said just request they fax it over to us. So I call the PCP and get someone who had no idea what was supposed to be done , so I had to explain it to him. My Dermo was another story. He is only in the office Mon-Wed. It is supposed to be till 3pm. I called at 2;10. NA. Called again at 2;30. NA. So I will not be able to get the records to the IDS until Monday. I call the PCP again and talk to someone different and they tell me the IDS needs to make a request for the records. This is all happening while I have a fever and every joint is killing me.
I apologize for the length but I just wanted for it all to be out there for the conspiracy theorists (of which I am one) . There may be some nefarious plan afoot with the tests. But that if it is happening it is happening at a higher level. The level of the interface of patient / doctor is completely broken. These idiots couldn’t pull on their underwear let alone pull off a conspiracy. I have received far more compassionate and competent care for far less money in India than in this country. Trust me no one wants Medicare for all.
So if you don’t see me around “now you know the rest of the story” I will see you on the other side
I have used mostly all of my 9 lives by now, mostly doing things I shouldn’t have enjoyed so much; it just seems unfortunate to contemplate succumbing to a turbo charged Chinese cold virus after all that undeserved luck. With the advice and information on this forum, it may, possibly, allow me to slip under a few more wires
Sorry, Chris, I was recalling a graphic for California, not the US as a whole. Apologies. Here is a link which includes the graphic I saw (though I saw it in a different article).
Thank you Chris for this explanation of the PCR test.
https://mapthenews.maps.arcgis.com/apps/opsdashboard/index.html#/5df19abcf8714bc590a3b143e14a548c
From this chart on the right hand side is the number of people testing positive on PCR tests in France (45 cycle) for a seven day period - with the seventh day dropping off as you go along. We were testing around 360 six weeks ago in our area, now we are below 80. If you click - on this same chart on the right-hand side - on the little arrow pointing left - you will get the percentage of réanimation ICU beds being used, all purposes, in each département. There are a few “hot spots” like Ardeche where there are 18 patients in ICU for 8 beds. Clearly not enough beds.
We have been duped by the misinformation regarding these tests - clearly a great number of people who are testing positive are not “contagious”. We will know early next year to what extent this second lockdown was a folly when the comparatives of previous year’s deaths versus 2020 are available.
https://www.theguardian.com/world/2020/dec/02/us-braces-for-covid-19-surge-thanksgiving-holiday
More than 100,000 hospitalisations, nearly 20,000 ICU patients and over 6,855 patients on ventilators (which seems a high proportion of ICU patients).
Muhamad
Sorry to hear about your ordeal. But please do stay on this side a bit longer and continue with your erudite commentary.
Just remember that there is no limit to human stupidity, and if we two legged lemmings all run off the cliff there will be other less destructive species to take our place.