Whether our new poster is the second coming of Frosty, or just another mind-controlled NPC like him… it doesn’t really matter. These factless defenders of the status quo narrative “”“Truth”“” tend to incite me to do better at presenting the actual science. Mr. Truth sets up these factless arguments is ways that actually make no sense. Nobody at PP.com every said ARDs wasn’t bad, or real, or that it does not lead to permanent damage and fibrosis. Indeed, we were talking about these things before most, and these realities drove our collective inquiry into the role that supplements and pharma drugs, mostly repurposed, could play in protecting us from the most damaging phase II and III effects of Covid-19 infection.
New poster Truth(ish) said;
Or maybe the coronavirus is not that dangerous and just take vitamin D and you will be fine. Wow, talk about uninformed. Good luck with that approach. Is it even worth trying to explain common sense to someone who just doesn't get it?Uninformed? Me? Us collectively? Let's talk Vitamin D, shall we? The more I learn, the more I tend to believe that, for most people who are not too old or otherwise suffering from co-morbidities, indeed if you take enough Vitamin D you will likely come out OK in the face of a Covid-19 infection. The big question is this; How much is enough? This is where it gets interesting. If you have not read the whole thing, I highly recommend anyone who is waivering on taking, or confused about dosing, to read the open letter regarding Vitamin D, now signed by over 200 MD's, PhD's, and MD/PhD's - I want to call attention to one particular passage;
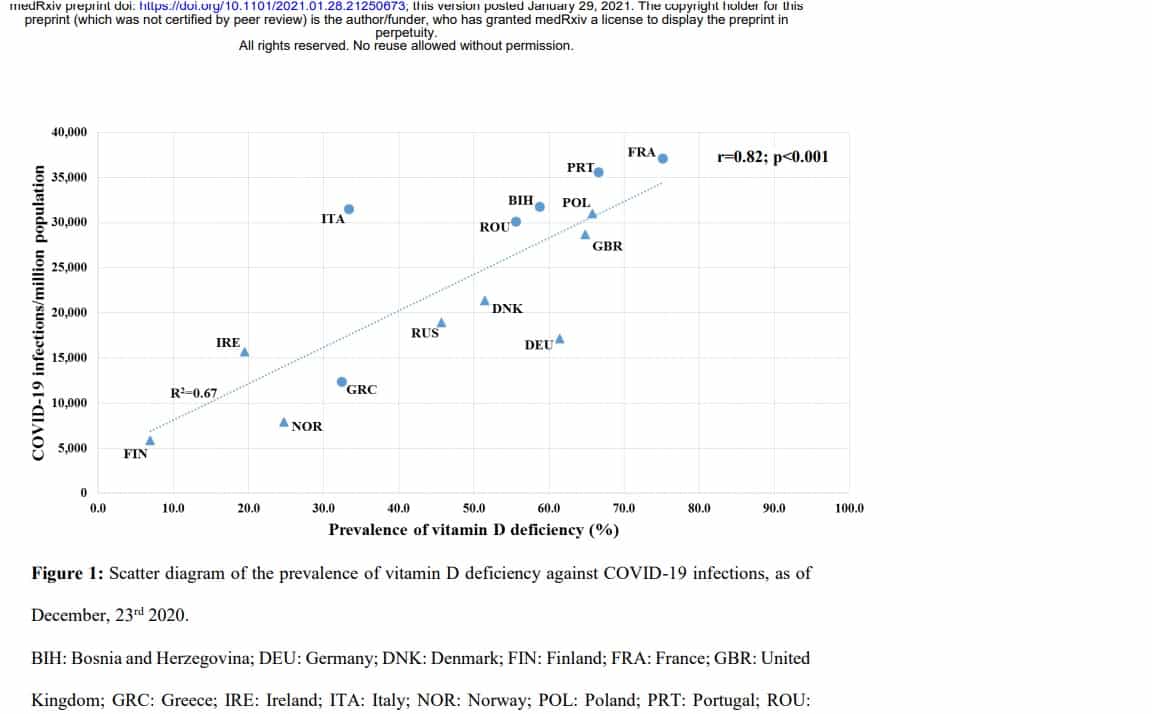
#VitaminDforAll: Over 200 Scientists and Doctors Call For Vitamin D To Combat COVID19 It has been shown that 3875 IU (97mcg) daily is required for 97.5% of people to reach 20ng/ml, and 6200 IU (155mcg) for 30ng/ml,4 intakes far above all national guidelines. Unfortunately, the report that set the US RDA included an admitted statistical error in which required intake was calculated to be ~10x too low.4 Numerous calls in the academic literature to raise official recommended intakes had not yet resulted in increases by the time SARS-CoV-2 arrived. Now, many papers indicate that vitamin D affects COVID-19 more strongly than most other health conditions, with increased risk at levels < 30ng/ml (75nmol/L) and severely greater risk < 20ng/ml (50nmol/L).1Got it? Not only do we see worse outcomes for those who are deficient in Vitamin D, the concepts of dosing on which the RDA is based are wrong by 10X! An order of magnitude! The document in the link is also educational in that most signatories list their personal dosing recommendation AND what they take themselves daily.. I didn't do the math, but you will see 5000 IU come up as being close to the mean recommendation. The letter argues the general case for linking Vitamin D deficiency to bad Covid-19 outcomes. More and more data comes out to help us see the relationship between Vitamin D and Covid-19 outcomes.. here is one of the latest, graphically; There is a final piece of this puzzle that I want to highlight - Vitamin D dosing vs sufficiency does not act in a linear fashion in the case of obesity. That is to say, whereas most pharmacokinetic dosing is roughly linear with body weight, Vitamin D is decidedly NOT. This then may be one of the main reasons that Obesity has proven to be a co-morbidity in relation to Covid-19 infection. Here's some data from a popular press (not scientific research) article from 2015;
https://www.vitalchoice.com/article/vitamin-d-rda-deemed-much-too-low Vitamin RDA also depends on weight The authors of a second paper call for a re-evaluation of the vitamin D RDA to account for body weight. Because body fat sequesters this fat-soluble vitamin, it takes more supplemental vitamin D to raise blood levels in overweight and obese people. The paper was authored by vitamin D experts from the University of Calgary, the Boston University School of Medicine, and the Harvard School of Public Health (Ekwaru JP et al. 2014). As they wrote, "Although differences in vitamin D by body mass index (BMI) and by absolute body weight have been reported [in eight other papers], the RDA does not consider either [factor].” Analysis of vitamin D intakes and levels in more than 20,000 people indicated that the current RDA of 600 IU is too low to achieve optimal vitamin D status. Indeed, the dose needed for overweight or obese individuals to reach optimal vitamin D levels is 12,000-20,000 IU. That's two to three times higher than the amount needed by a normal weight individual, and four to five times higher than the maximum intake currently recommended (4,000 IU per day). With a significant portion of the US population being overweight or obese, the findings have potentially serious implications. The new analysis also showed that vitamin D supplementation was safe up to 20,000 IU per day, even for normal weight people. "We recommend clinical guidelines for vitamin D supplementation be specific for normal weight, overweight and obese individuals,” they concluded.If we look we can see that there is a whole canon of research discussing the relation to, and implications of, Vitamin D deficiency in the obese. Why the heck haven't we seen more on this subject by our governmental health authorities? Why have they missed this obvious, smoking gun when it comes to susceptibility to Covid-19 and Vitamin D, especially in the case of obesity, where Vitamin D needs are higher than would be expected given a linear dose vs weight extrapolation model? I think we know. I'll end with this link from mid-2019;
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6780345/ Vitamin D Deficiency: Consequence or Cause of Obesity? Obesity is defined as an excess amount of body fat and represents a significant health problem worldwide. High prevalence of vitamin D (VD) deficiency in obese subjects is a well-documented finding, most probably due to volumetric dilution into the greater volumes of fat, serum, liver, and muscle,