As for the risk groups, you left off one of the biggest: age.
You didn't read the IFR document I attached? This lays out - specifically - age-stratified risk levels. You were opining that COVID had a 1% IFR. I said this was true only if you were >= 65 years old. It is not true if you were (say) 20, as those poor kids who were coerced into taking the not-so-safe-and-effective shot.
We also have a very sedentary and obese population. I would rather not write all of those people off. Now, I agree with you 100% that getting the vaccine while maintaining an unhealthy lifestyle (to the extent that one has control over that) would be foolish.
Yep. We agree. Obesity and sedentary lifestyles cannot be overcome via vaccination. One might argue that losing your fat, and engaging in activity, are more protective for you - for a lot more than just COVID19 - than even the best case of the vaccines as they appeared on day #1. If you want to remain obese and immobile - then it might make sense to take the shot. Maybe.
A few years ago, I got severely deficient in vitamin D without knowing it. I'm active, spend a LOT of time outdoors, and eat a lot of wild game. My doctor was very surprised, and so was I. 4000 IU in drops on my toast or cereal in the morning brought me to normal within a few months. Then COVID hit. Dodged a bullet there, maybe, I'll never know.
I suspect there is a lot more vitamin D deficiency than most people realize, but it looks from what I've read that there is not a whole lot of benefit in mega doses, especially after infection.
Form of vitamin D does matter. There were some really interesting results, early on, of using the active form Vitamin D (calcifediol). The normal D3 takes time to work. The calcifediol form is processed by the body immediately. Using it on hospitalized patients at admission cut mortality by 70%.
As you point out, most people are deficient. As a result, the "standard IFR" numbers assume most people are vitamin D deficient. Therefore, if you aren't deficient, your improved vitamin D levels will reduce your IFR as you might expect.
Same for activity.
Same for obesity.
All of these prevention techniques are useful across a wide range of illnesses - including cancer (for vitamin D). They are - in aggregate, much safer and more effective than a brand-new vaccine which has no long term evidence of safety or efficacy.
I mean - good luck with the boosters and all. Let's hope there aren't long term ill effects.
I'll stick with activity, normal BMI, vitamin D sufficiency (as you point out, you MUST test - my vit-D level is ~60 ng/ml), and - super important - early outpatient treatment, which reduces hospitalization and death by 95%.
I am much more clear about the factors that go into my own health today than I was 2 years ago. For that, I thank myself (Doctor Yourself!), as well as everyone here at this site for their contributions.
Doctor Yourself. Early Treatment Saves Lives.
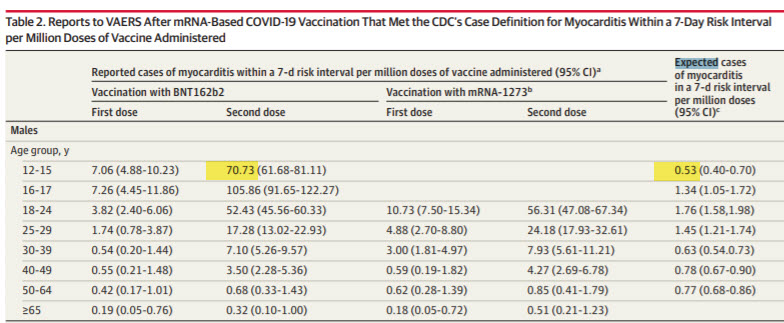
You're right, that is what Chris said. My bad on that. But now that I went back and read it, I cannot find anything in the paper that supports that number. It is not given as far as I can see, and there don't seem to be any background numbers presented from which one could calculate it.
They calculated the expected number of myocarditis events during a 7-day window and compared that to their findings in a seven-day window after both the first and then the second shot.
70.73/0.53 = 133.45
What other data do you have or know of to help me prepare for my next meeting with the cardiologist?
Yes. Tons.
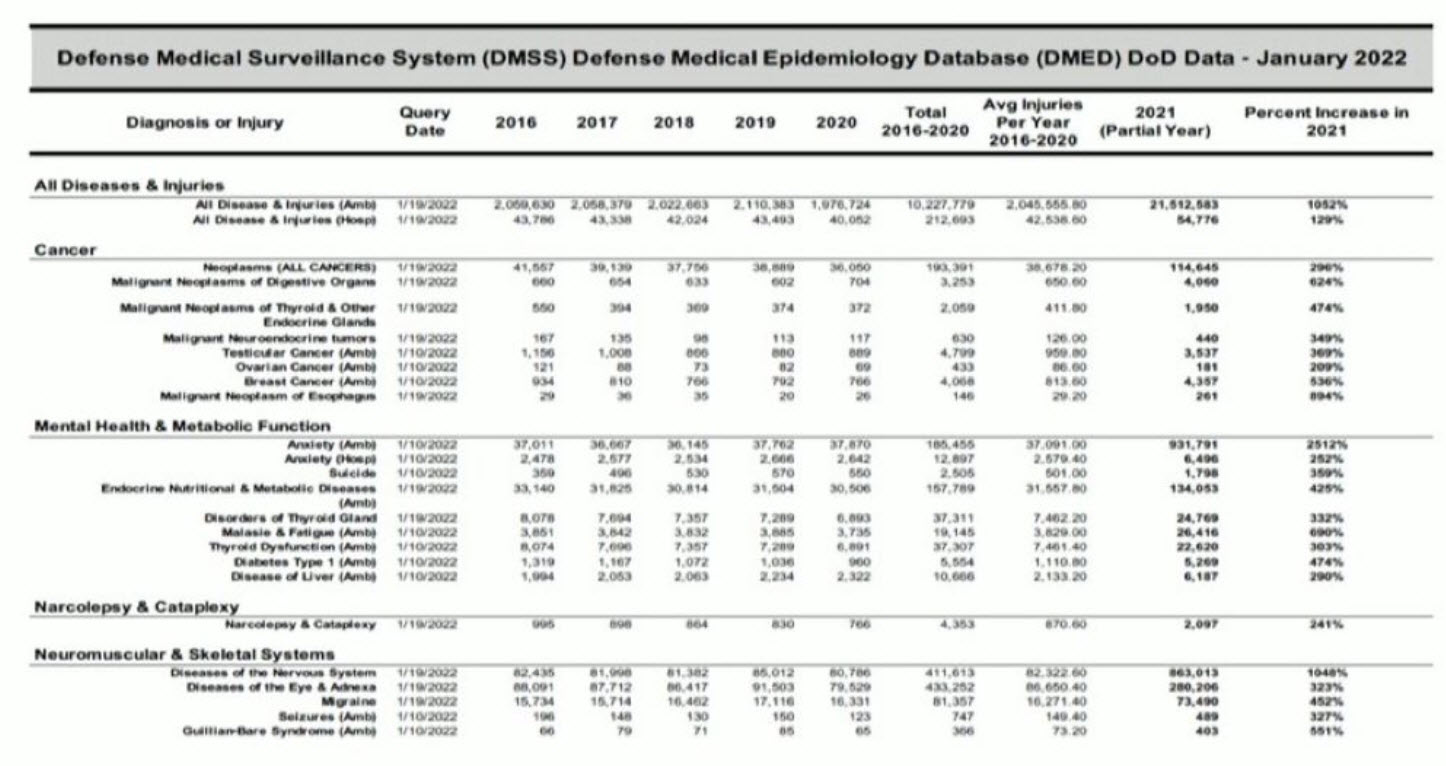
I'd start with the DMED releases.
Here's a fuzzy table, but it shows a whopping 1052% increase all diseases and injuries in the military in 2021 compared to the five-year prior baseline.
Here's a summary:
279% SPIKE in Miscarriages
487% SPIKE in Breast Cancer
1048% SPIKE in the Nervous System
155% SPIKE in Birth Defects
350% SPIKE in Male Infertility
369% SPIKE in Testicular Cancer
2181% SPIKE in Hypertension
664% SPIKE in Malignant Neoplasms
680% SPIKE in Multiple Sclerosis
551% SPIKE in Guillain-Barre Syndrome
468% SPIKE in Pulmonary Embolism
302% SPIKE in Tachycardia
452% SPIKE in Migraines
471% SPIKE in Female Infertility
437% SPIKE in Ovarian Dysfunction
269% SPIKE in Myocardial infarction
291% SPIKE in Bell’s palsy
467% SPIKE in Pulmonary Embolism
You can download the base data here: https://renz-law.com/dmed-data/
I'd next go and peruse all the charts and graphs at Renz Law here: https://renz-law.com/attorney-tom-renz-whistleblowers-dmed-defense-medical-epidemiology-database-reveals-incredibly-disturbing-spikes-in-diseases-infertility-injuries-across-the-board-after-the-military-was-forced-to/
Then I'd give him the German BKK insurance data: https://www.eugyppius.com/p/german-public-health-insurer-vaccine?utm_source=substack&utm_campaign=post_embed&utm_medium=web
And: https://roundingtheearth.substack.com/p/vaccine-induced-mortality-part-9
Finally ask your doc to explain these results be sure to ask them if "a p-value of less than 0.0001 is significant?"
A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products
Jessica Rose PhD, MSc, BSc and Peter A. McCullough MD, MPH
Nov 2, 2021
1,104
129
Abstract
Following the global rollout and administration of the Pfizer Inc./BioNTech BNT162b2 and Moderna mRNA-1273 vaccines on December 17, 2020, in the United States, and of the Janssen Ad26.COV2.S product on April 1st, 2021, in an unprecedented manner, hundreds of thousands of individuals have reported adverse events (AEs) using the Vaccine Adverse Events Reports System (VAERS).
We used VAERS data to examine cardiac AEs, primarily myocarditis, reported following injection of the first or second dose of the COVID-19 injectable products. Myocarditis rates reported in VAERS were significantly higher in youths between the ages of 13 to 23 (p<0.0001) with ∼80% occurring in males.
Within 8 weeks of the public offering of COVID-19 products to the 12-15-year-old age group, we found 19 times the expected number of myocarditis cases in the vaccination volunteers over background myocarditis rates for this age group. In addition, a 5-fold increase in myocarditis rate was observed subsequent to dose 2 as opposed to dose 1 in 15-year-old males.
A total of 67% of all cases occurred with BNT162b2. Of the total myocarditis AE reports, 6 individuals died (1.1%) and of these, 2 were under 20 years of age - 1 was 13. These findings suggest a markedly higher risk for myocarditis subsequent to COVID-19 injectable product use than for other known vaccines, and this is well above known background rates for myocarditis.
COVID-19 injectable products are novel and have a genetic, pathogenic mechanism of action causing uncontrolled expression of SARS-CoV-2 spike protein within human cells. When you combine this fact with the temporal relationship of AE occurrence and reporting, biological plausibility of cause and effect, and the fact that these data are internally and externally consistent with emerging sources of clinical data, it supports a conclusion that the COVID-19 biological products are deterministic for the myocarditis cases observed after injection.
Keywords
SARS-CoV-2, COVID-19, myocarditis, VAERS, adverse events (AEs), COVID-19-Injection-Related Myocarditis (CIRM)
We have not been “failed” by medical institutions and government agencies. This is so far beyond gross incompetence. This has to be deliberate, unfortunately for us.