There’s a reason we’ve re-directed so much of our attention towards reporting on and trying to understand the novel coronavirus (covid-19) that originated in Wuhan, China in December.
The heart of our approach is to be “systems thinkers.”
“Learn how to see. Realize that everything connects to everything else”~ Leonardo Davinci
We don’t see the economy as a closed ecosystem to be analyzed and understood all on its own. It’s connected to energy flows, especially oil. So we investigate those, too, with an eye towards working out how fossil fuels’ eventual dwindling will impact an economic system that is utterly dependent on perpetual growth.
Without a healthy planet, without intact and functioning ecological systems, nothing matters in either the economy or the energy markets. Both impact the ecological world And vice versa. So we analyze and report on the environment, too.
Which is why we’re confident in claiming that humanity is now facing its greatest threat. Our current path of depleting our essential resources at an accelerating rate in the pursuit of “more growth” is both unsustainable and self-destructive.
So here we are, with a global economy that’s very cost-efficient but not resilient. It’s wonderful that Walmart has worked out how to order a new tube of toothpaste from China the second one is pulled off a shelf in Topeka, KS. But that means there is no deep storage to draw upon in times of disruption to the status quo. No warehouses stocked with 12 months of future goods. Just a brilliantly-complicated supply chain thousands of miles long that has to work perfectly for things to keep running.
As an example that drives home this point: we learned during the 2011 earthquake in Japan that there was just one single factory making a necessary polymer gel for the odd-shaped lithium batteries used in smartphones and iPods. There was no backup factory.
We watched closely during that enormous crisis (which also spawned the Fukushima nuclear disaster) as electronics companies scrambled to triage their remaining supplies and attempt to find new sources. It was very touch and go. Vast portions of the battery-fueled electronic industry came within a whisker of simply shutting down production – all for want of an esoteric polymer gel.
Yes, the most cost-effective way to make that gel was to house it all in a single plant. But it made no sense from a redundancy and resilience standpoint.
And did ‘we’ learn from that experience? Nope.
Supply Chain Armageddon
The global economy is more interdependent than ever. Its supply chains are built on a huge network of dependencies with many ‘single points of failure’ strung along its many branches.Can anybody predict what will happen next? No.
But we’re already seeing early failures as Chinese plants, factories and ports sit idle from the country’s massive quarantine efforts:
China set to lose out on production of 1M vehicles as coronavirus closes car plantsChina exports about $70 billion worth of car parts and accessories globally, with roughly 20 percent going to the U.S.
Feb. 5, 2020, 4:32 PM EST
By Paul A. Eisenstein
China could suffer the loss of a million vehicles worth of production as factories in its crucial automotive industry remain shuttered until at least next week — and likely longer in Wuhan, the “motor city” at the center of the coronavirus outbreak.
With more than 24,000 people infected, the impact of the highly contagious disease is also beginning to be felt by automakers in other parts of the world. Hyundai is suspending production in its South Korean plants because of a shortage of Chinese-made parts, and even European car manufacturers could be hit: Volkswagen and BMW could see a dip of 5 percent in their earnings for the first half of 2020, according to research firm Bernstein.
We’re predicting that these auto shutdowns are just beginning. All it takes is a single component to be unavailable and the entire line has to be shut down.
Is China the sole source for many critical components in the auto industry? Absolutely.
Here’s an inside view:
On Monday, Steve Banker and I had the opportunity to speak with Razat Gaurav, CEO of Llamasoft. Razat had some interesting takes on the outbreak, especially as it relates to the automotive and pharmaceutical supply chains. On average it takes 30,000 parts to make a finished automobile.Due to the virus, production facilities have already indicated that they will have lower than normal parts volumes. This has left companies scrambling to make contingency plans. During my conversation with Razat, he mentioned that inventories for most of these automotive parts are managed on a lean just-in-time basis.
This means that, on average, companies have anywhere between two and twelve weeks of buffer inventory on-hand for automotive parts. As production volumes are decreasing, this has the potential to cause quite the global shortage of parts. The buffer inventory will only last so long, and once the pre-holiday supply runs dry, the industry is going to be in serious trouble. According to Gaurav: “Most OEMs single source components for new vehicles and China is a large supplier of those.”
“Single sourcing” is exactly what it implies. There’s a single factory somewhere churning out a single component that is absolutely vital to make a motorized vehicle. If that factory goes away for any length of time, a new source has to be identified or – worse, from a time and cost standpoint – built from scratch.
But this vulnerability to China-dependent supply chains is by no means unique to the auto industry:
Last month, the U.S.-China Economic and Security Review Commission held a hearing on the United States’ growing reliance on China's pharmaceutical products. The topic reminded me of a spirited discussion described in Bob Woodward’s book, Fear: Trump in the White House.In the discussion, Gary Cohn, then chief economic advisor to President Trump, argued against a trade war with China by invoking a Department of Commerce study that found that 97 percent of all antibiotics in the United States came from China.
That’s as close to a ‘sole source’ as you can get.
And to put the cherry on top: guess the name of the region in China responsible for producing all if these antibiotics? Yep, Hubei province. With Wuhan its most important production hub.
Can we find another source for our generic drugs and antibiotics? India, possibly. But here again we run into the same global interdependency issue:
Another industry that is feeling the impact of the coronavirus is the pharmaceutical industry. The average buffer inventory for the pharmaceutical industry is between three and six months. However, this does not tell the full story. Gaurav mentioned that China is responsible for producing 40 percent of the active pharmaceutical ingredients (APIs) for the pharmaceutical world.Additionally, China supplies 80 percent of key starting materials (KSM’s), which are the chemicals in APIs, to India. Put together, this represents 70 percent of all APIs across the world.
India’s production is directly tied to uninterrupted supply from China:
Indian generic drugmakers may face supply shortages from China if coronavirus drags onFeb 13 (Reuters) - Shortages and potential price increases of generic drugs from India loom if the coronavirus outbreak disrupts suppliers of pharmaceutical ingredients in China past April, according to industry experts.
An important supplier of generic drugs to the world, Indian companies procure almost 70% of the active pharmaceutical ingredients (APIs) for their medicines from China.
India’s generic drugmakers say they currently have enough API supplies from China to cover their operations for up to about three months.
“We are comfortably placed with eight to 10 weeks of key inventory in place,” said Debabrata Chakravorty, head of global sourcing and supply chain for Lupin Ltd, adding that the company does have some local suppliers for ingredients.
Sun Pharmaceuticals Industries Ltd said it has sufficient inventory of API and raw materials for the short term and has not seen any major disruption in supplies at the moment.
The Indian drugmaker, however, said supply has been impacted for a few API products and the company is closely monitoring the situation. It did not identify the products.
India supplies nearly a third of medicines sold in the United States, the world’s largest and most lucrative healthcare market.
(Source)
Is this a huge concern? Of course it is.
If you’re dependent in any way on prescription drugs, it would be entirely rational to chase down whether those come from China or India and, if they are, begin talks with your doctor about alternatives or what to do if supplies get pinched.
A Fast-Moving Situation
Look, we entirely get why the authorities and media are downplaying the covid-19 pandemic. We really do. They feel the need to manage the crisis, which means managing the public narrative.But c’mon. Does it make any sense for Apple’s stock price to be up while its main Foxconn manufacturing facility is all but completely shuttered?
Fewer iPhones and Airpods being made should equate with lower future earnings and thus a lower stock price. But no, AAPL is up handily over the past month:

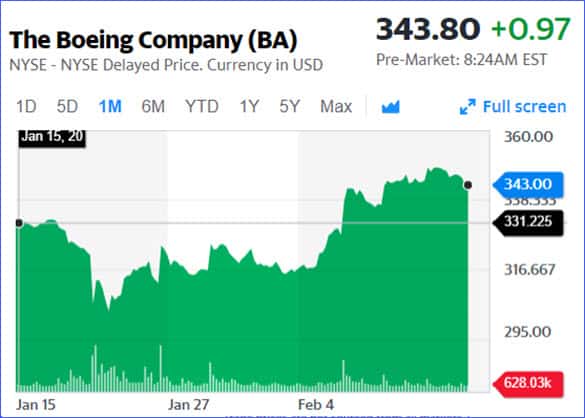
And this is even crazier. Does it make ANY sense for Boeing’s stock to be up $12 over the past month? As it reported its first year (2019) of NEGATIVE orders and a completely order-free January (2020)? No, of course not.
But those are the sorts of ‘signals’ that the officials believe have to be sent in order to keep the masses from catching on that something really concerning is happening.
Unfortunately, such signals work on the masses. Higher stock prices send a powerful comforting message that “all is well”.
But prudent critical thinkers, which defines those in the Peak Prosperity tribe, can readily see through the ruse and get busy preparing themselves for what’s coming.
It's Time For Action
The situation with covid-19 is fluid, and fast-moving. Staying on top of the breaking developments and making sense of them for you is our primary job.But information without informed action is useless.
After all, knowing something concerning but then doing nothing about it is merely cause for anxiety if not alarm.
The only ways to remain calm and protect your loved ones from the threat of this pandemic are rooted in taking smart action.
Yes, we can all hope this blows over. We sincerely wish the macro-planners all the best in shaping the narrative and keeping the macro economy somehow functioning and glued together.
But we’re going to prepare as best we can, here at our micro level because that’s our duty to ourselves, to our families, and to our communities.
Creating A Resilient Defense Against The Coronavirus
This is a huge moment in history. The first global pandemic at a time when the world economy is sole-sourced and completely interdependent.Nobody can predict what will happen next. Autos, drugs…who knows what the next industry to stumble will be?
Given the ridiculously high rate of infectivity of covid-19 there’s really no chance of stopping its spread. The rate is now just a equation of time, luck, and official actions to aggressively isolate and quarantine infected individuals and communities.
Our position affords us many experienced contacts with experts throughout the world, and those we know with deep medical training are preparing the most aggressively right now. This outbreak has their full attention; and that informs us that it should have ours, too.
Which is why our advice is to get busy preparing yourself now.
Last week we issued the guide How We’re Personally Preparing For The Coronavirus to our premium subscribers. It’s a great resource providing specific recommendations for prevention and treatment.
Today, we’re releasing an expanded companion guide A Resilient Defense Against The Coronavirus, again for our premium members.
Particularly useful for those who have recently found their way to PeakProsperity.com, it offers both a valuable framework to use in preparing for any disaster (including pandemics) and then details out specific action steps to take today across all aspects of your life (i.e., not just health & hygiene) against a coronavirus outbreak in your local area.
Click here to read this report (free executive summary, enrollment required for full access).
This is a companion discussion topic for the original entry at https://peakprosperity.com/why-covid-19-demands-our-full-attention/